eduo
visual
Gastrointestinal
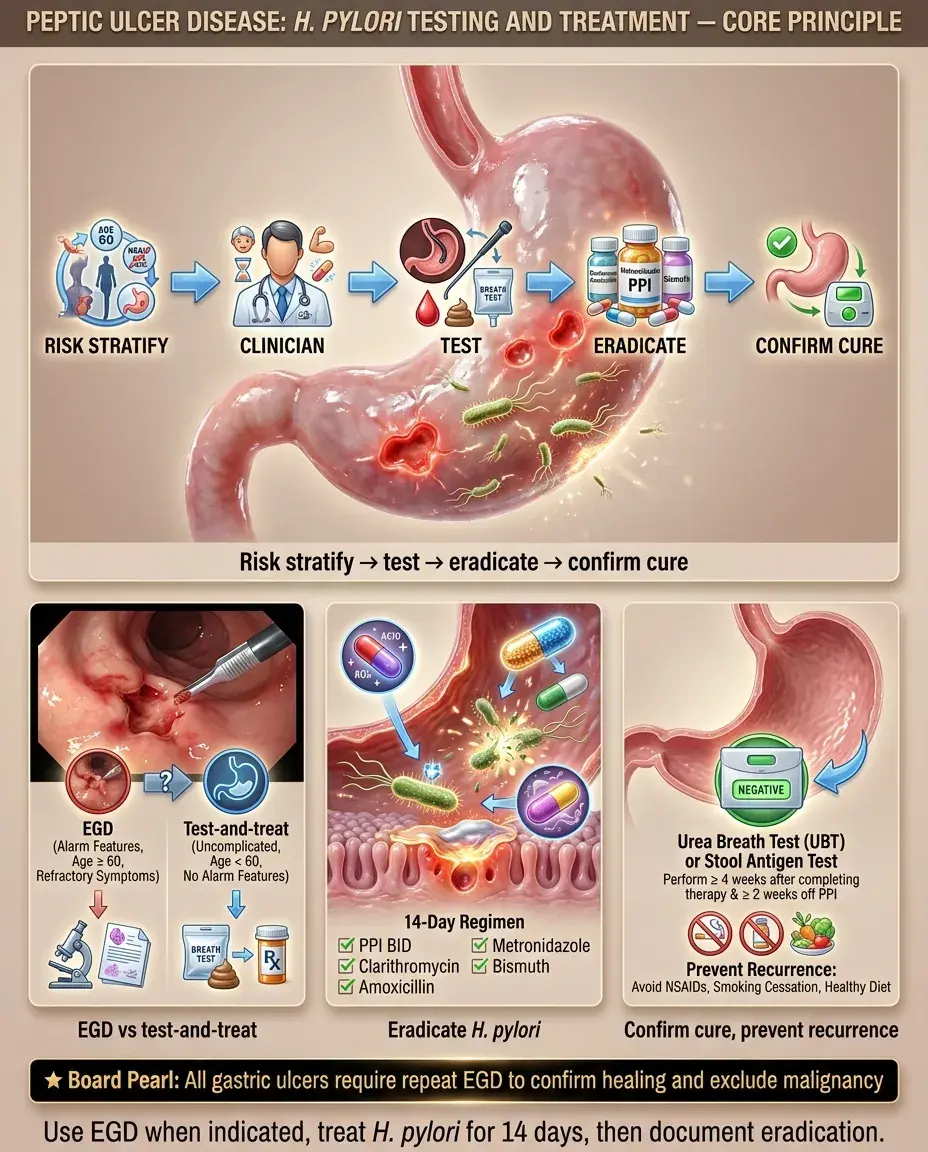
Peptic ulcer disease: H. pylori testing and treatment
PUD refers to mucosal defects in the stomach or duodenum that extend through the muscularis mucosae, most commonly caused by Helicobacter pylori infection or NSAID use.
— Gnawing/burning epigastric pain, often nocturnal
— Pain improved (duodenal) or worsened (gastric) by eating
— History of NSAID/aspirin use, smoking, or prior H. pylori infection
— Nausea, early satiety, bloating
Board pearl: All patients with documented PUD must be tested for H. pylori — eradication heals ulcers and dramatically reduces recurrence from ~80% to <5%.

Duodenal ulcer pattern:
Gastric ulcer pattern:
Critical history elements:
Next best step: Ask about alarm features (see chunk 4) in every patient with dyspepsia — they determine whether to proceed directly to endoscopy vs noninvasive H. pylori testing.

Uncomplicated PUD:
Signs suggesting complications:
Board pearl: Succussion splash (sloshing sound with gentle rocking) suggests retained gastric contents → think GOO from chronic PUD or malignancy.

Alarm features mandating esophagogastroduodenoscopy (EGD):
Approach without alarm features (age <60):
If EGD performed:
Key distinction: Duodenal ulcers rarely need follow-up EGD; gastric ulcers always need repeat EGD to confirm healing and exclude cancer.

Noninvasive tests:
Invasive tests (during EGD):
Critical pre-test requirements:
Board pearl: Serology is the only test unaffected by PPI/antibiotic use but cannot be used for test-of-cure because IgG remains positive long after eradication.

First-line regimen selection depends on local clarithromycin resistance (<15% → triple OK; ≥15% or unknown → quadruple preferred):
Bismuth quadruple therapy (preferred if resistance unknown):
Clarithromycin-based triple therapy (only if local resistance <15% AND no prior macrolide exposure):
Key principles:
Next best step: Before prescribing, ask about penicillin allergy and prior macrolide exposure — these change the regimen.

Concomitant therapy (increasingly used first-line):
Levofloxacin-based triple therapy (salvage/second-line):
Rifabutin-based triple therapy (third-line/refractory):
General salvage principles:
Board pearl: After first-line failure, switch to a regimen with completely different antibiotics — do not repeat the same class.

PUD management overview:
1. Test for H. pylori → eradicate if positive
2. Discontinue NSAIDs if possible
3. PPI therapy to heal ulcer:
— DU: PPI × 4–8 weeks
— GU: PPI × 8–12 weeks
4. Confirm H. pylori eradication (test-of-cure)
5. GU: repeat EGD at 8–12 weeks to document healing
If H. pylori-negative and NSAID-negative:
PPI dosing for ulcer healing:
Key distinction: NSAID-related ulcers require NSAID cessation as the primary intervention; H. pylori eradication alone does not heal NSAID-induced ulcers if the drug is continued.

Pregnancy:
Pediatric considerations:
Elderly:
Board pearl: In pregnancy, defer H. pylori eradication if possible; bismuth and tetracycline are absolutely contraindicated.

Risk factors for NSAID-induced PUD:
Gastroprotection strategies:
Aspirin users:
Key distinction: H. pylori and NSAIDs are independent, synergistic risk factors. Eradicating H. pylori reduces but does not eliminate NSAID ulcer risk — PPI co-therapy is still needed in high-risk patients on chronic NSAIDs.
Next best step: Before starting long-term NSAID therapy in a patient with PUD history → test for H. pylori, eradicate if positive, AND add PPI.

PUD is the most common cause of upper GI bleeding (UGIB).
Initial management:
EGD timing:
Forrest classification (endoscopic findings guiding rebleeding risk):
Board pearl: IV PPI infusion is started empirically before EGD in suspected bleeding PUD — it stabilizes clots and reduces the need for endoscopic intervention.

Perforation:
Gastric outlet obstruction (GOO):
Board pearl: Anterior DU → perforation; posterior DU → hemorrhage (gastroduodenal artery erosion).

Functional dyspepsia:
Gastric cancer:
Zollinger-Ellison syndrome (ZES):
Key distinction: Isolated gastric ulcer that fails to heal after 12 weeks of PPI + H. pylori eradication → biopsy to exclude malignancy or consider ZES.

H. pylori-related PUD:
NSAID-related PUD:
Both present:
Board pearl: NSAID ulcers are commonly asymptomatic until complications occur — this is why gastroprophylaxis with PPI is recommended in high-risk patients on chronic NSAIDs.

Confirming H. pylori eradication:
Follow-up EGD:
If eradication fails:
Next best step: After completing H. pylori therapy, wait ≥4 weeks off antibiotics and ≥2 weeks off PPIs before performing UBT or stool antigen for test-of-cure.

H. pylori screening indications (even without active PUD):
Long-term PPI monitoring (if ongoing PPI needed):
Prevention of PUD recurrence:
Board pearl: H. pylori eradication in gastric MALT lymphoma achieves complete remission in ~75–80% of localized (stage I) cases — chemotherapy may not be needed.

Informed consent and shared decision-making:
Antibiotic stewardship:
Medication safety:
Patient adherence:
Board pearl: Nonadherence is the most common cause of H. pylori treatment failure — address it before changing antibiotics.

Board pearl: H. pylori ↑ risk of both gastric adenocarcinoma and MALT lymphoma but is inversely associated with esophageal adenocarcinoma and GERD.