eduo
visual
Infectious Disease
Parasitic infections: malaria, toxoplasmosis
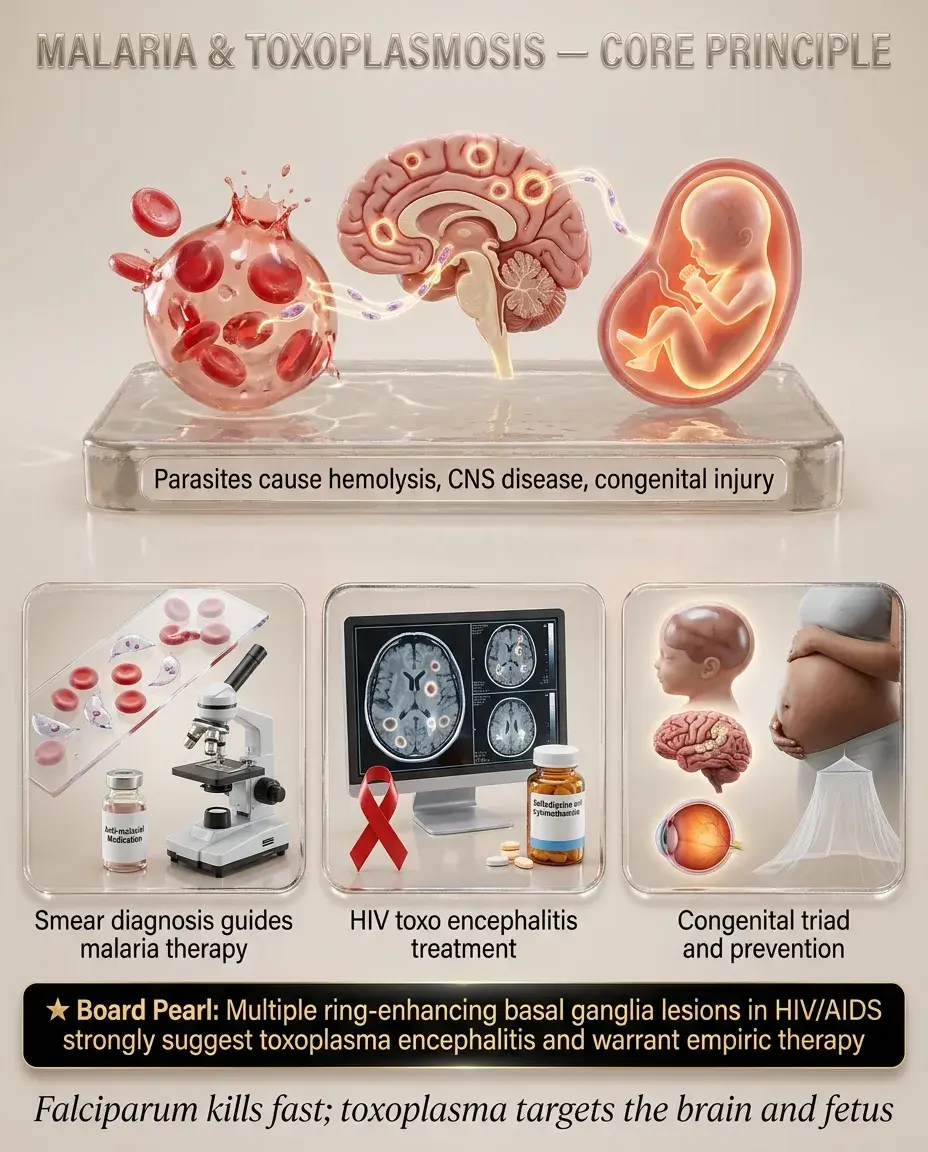
Malaria → Plasmodium spp. transmitted by female Anopheles mosquito → cyclical erythrocyte invasion and lysis → febrile hemolytic illness. Five species: P. falciparum (most lethal), P. vivax, P. ovale (both form hypnozoites), P. malariae, P. knowlesi.
Toxoplasmosis → Toxoplasma gondii, obligate intracellular protozoan → acquired via cat feces (oocysts), undercooked meat (tissue cysts), or transplacental transmission. Usually latent in immunocompetent hosts; reactivates with CD4 < 100.
Board pearl: Any fever in a returning traveler = malaria until proven otherwise. Delay in diagnosis of P. falciparum → rapid mortality.

— 48-hr cycle (tertian): P. falciparum, P. vivax, P. ovale
— 72-hr cycle (quartan): P. malariae
— Periodicity often absent early in disease
Critical history:
— Travel to endemic area within past 12 months (P. falciparum usually within 1 month; P. vivax/ovale can relapse months–years later from hepatic hypnozoites)
— Chemoprophylaxis use and adherence
— Prior malaria episodes
— Sickle cell trait (protective — ↓ severe malaria)
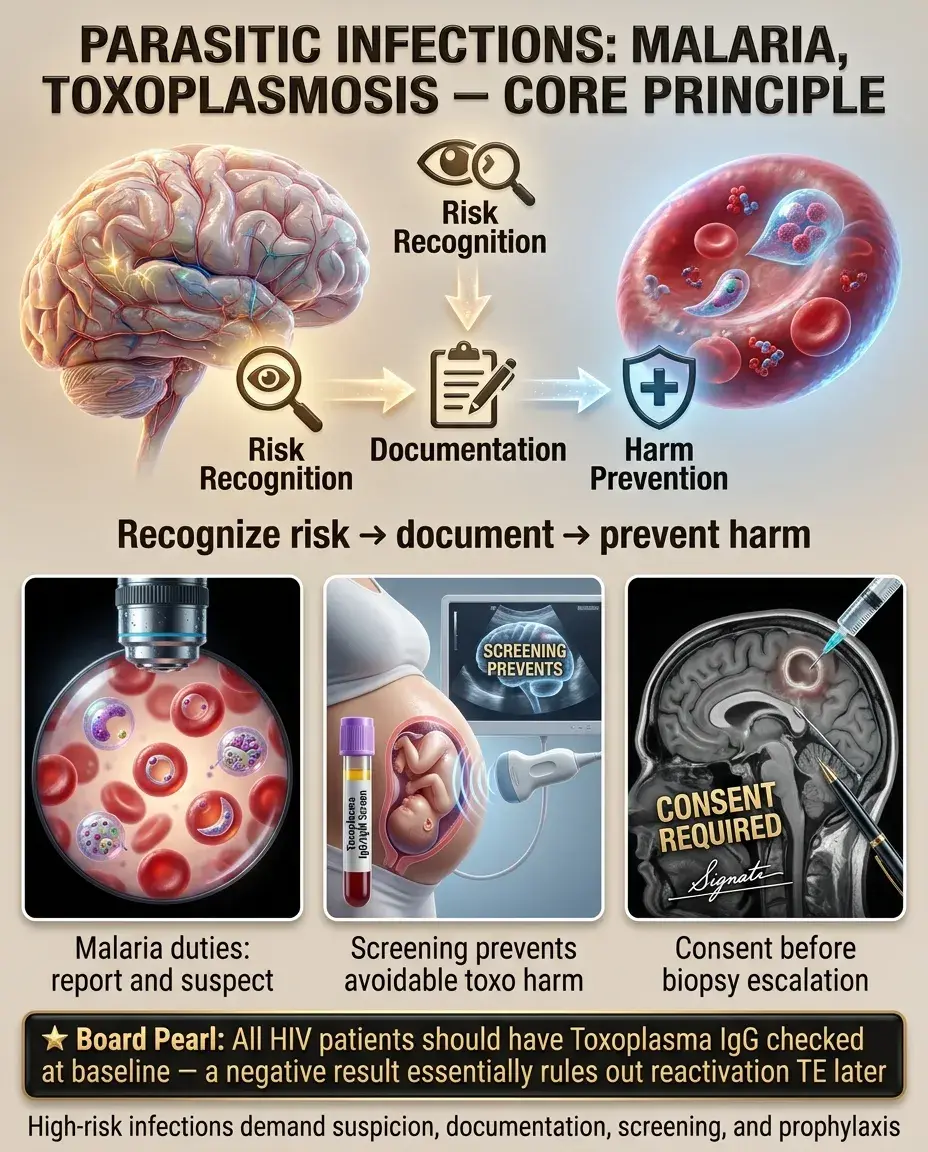
Next best step: Obtain thick and thin blood smears STAT in any febrile returning traveler.

Immunocompetent host:
Immunocompromised (HIV, CD4 < 100):
Congenital toxoplasmosis (classic triad):
Ocular toxoplasmosis:
Board pearl: Ring-enhancing brain lesions + HIV + CD4 < 100 + positive Toxoplasma IgG → empiric treatment for TE before biopsy.

— Thick smear: ↑ sensitivity (detects parasitemia)
— Thin smear: species identification and parasitemia quantification (%)
— If initial smear negative → repeat every 12–24 hrs × 3 before ruling out
— Useful for quick triage but does not quantify parasitemia
— False negatives with low parasitemia or HRP-2 gene deletions
Key distinction: Thrombocytopenia + fever + travel = think malaria. Thrombocytopenia is present in >80% of malaria cases and is a strong clue on board exams.

Immunocompetent:
— IgG positive alone → past infection/latency
— IgM positive + IgG negative or rising → acute infection
— IgG avidity testing: high avidity = infection >12–16 weeks ago (useful in pregnancy to date infection)
Toxoplasmic encephalitis (HIV):
— IgG negative makes TE very unlikely
Congenital:
Board pearl: High IgG avidity in a pregnant woman = infection occurred months ago → low risk to current fetus.

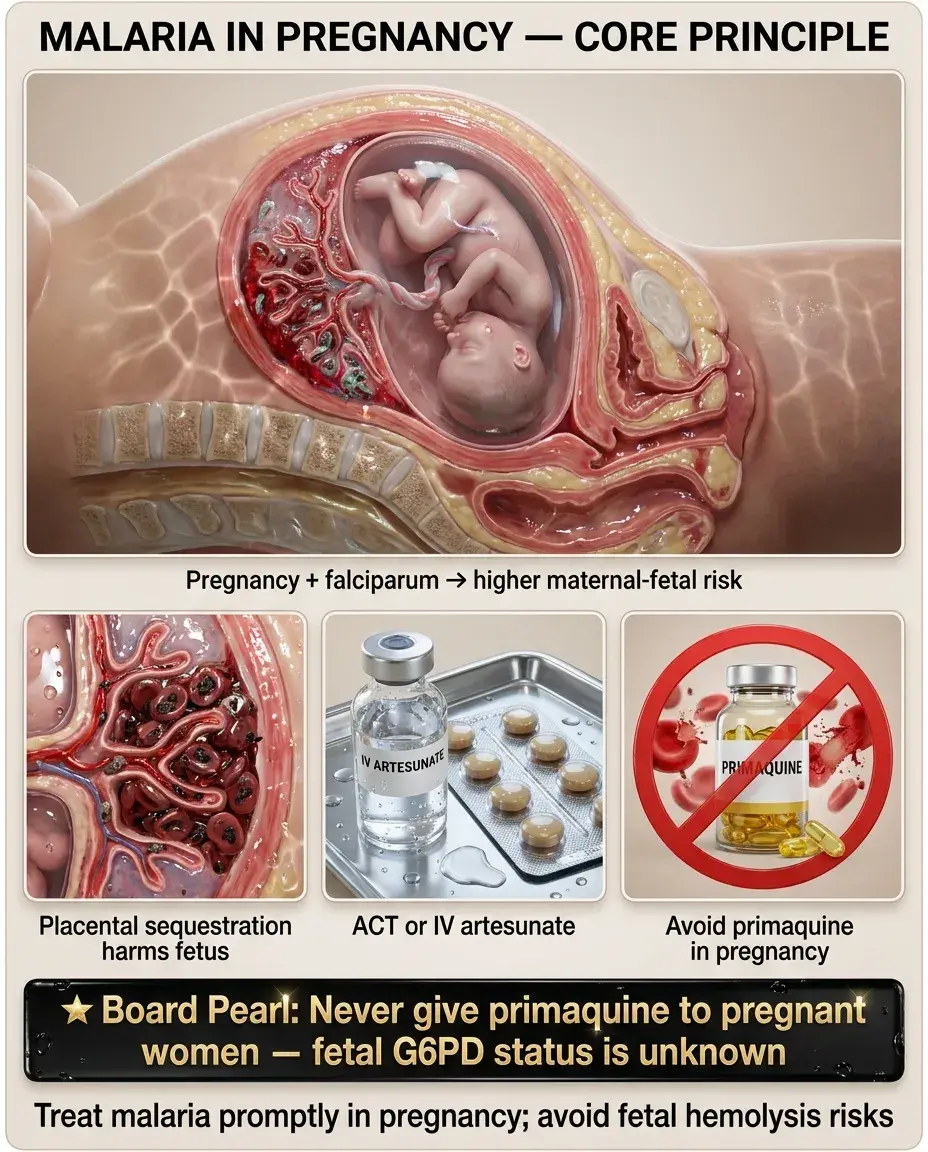
— Artemisinin-based combination therapy (ACT): artemether-lumefantrine (Coartem) — oral, well-tolerated
— Alternative: atovaquone-proguanil (Malarone)
— Chloroquine phosphate (oral)
— Chloroquine (still effective in most areas; resistance emerging in parts of Indonesia/Papua New Guinea)
— PLUS primaquine × 14 days (radical cure to eliminate hepatic hypnozoites)
— Must check G6PD before primaquine → hemolytic anemia in G6PD-deficient patients
— Alternative to primaquine: tafenoquine (single dose, also requires G6PD testing)
Board pearl: Primaquine kills hypnozoites (P. vivax/ovale) — without it, relapse will occur. Always test G6PD first.

Criteria for severe malaria (P. falciparum):
Treatment:
— Available in the U.S. via CDC
— Superior to IV quinidine in reducing mortality (SEAQUAMAT & AQUAMAT trials)
— Transition to oral ACT once patient can tolerate PO and parasitemia < 1%
— Requires cardiac monitoring (QT prolongation risk)
— Monitor blood glucose (quinidine stimulates insulin release → hypoglycemia)
Supportive care:
Next best step: Severe malaria with altered mental status → IV artesunate immediately; do not wait for species confirmation.

Toxoplasmic encephalitis (HIV/AIDS):
— Leucovorin prevents bone marrow suppression from pyrimethamine (folate antagonist)
— Pyrimethamine + clindamycin + leucovorin if sulfa allergy
— TMP-SMX is an alternative regimen with good CNS penetration
— Same drugs at reduced doses until CD4 > 200 × ≥6 months on ART
Immunocompetent lymphadenitis:
Ocular toxoplasmosis:
Board pearl: Leucovorin (folinic acid) does NOT reduce antiparasitic efficacy — it selectively rescues mammalian folate metabolism while Toxoplasma cannot use it.

Treatment:
— Quinine + clindamycin is alternative, especially in 1st trimester if ACT unavailable
Contraindicated in pregnancy:
— Defer hypnozoite treatment until after delivery + G6PD testing
Chemoprophylaxis in pregnancy:
Board pearl: Never give primaquine to pregnant women — fetal G6PD status is unknown.
Congenital toxoplasmosis:
Maternal treatment to reduce vertical transmission:
— Concentrates in placenta; reduces transmission ~60%
— Pyrimethamine is teratogenic in 1st trimester → avoid before week 18
Neonatal treatment:
Board pearl: Toxoplasma intracranial calcifications are diffuse/scattered (vs. CMV which causes periventricular calcifications).

— Mechanism: parasitized RBCs adhere to cerebral microvasculature (cytoadherence via PfEMP-1)
— Mortality 15–20% even with treatment; survivors may have neurologic sequelae
— Associated with G6PD deficiency + oxidant stress or quinine use
— Monitor glucose every 4–6 hours during treatment
Next best step: ICU admission for any patient meeting severe malaria criteria; start IV artesunate without delay.

— If untreated → herniation, death
— Seizures: manage with antiepileptics; mass effect may require corticosteroids (dexamethasone) for edema
— Immune reconstitution inflammatory syndrome (IRIS) after ART initiation: paradoxical worsening of TE due to recovering immune response → continue anti-Toxoplasma therapy + consider steroids
— Pneumonitis, myocarditis, hepatitis — seen in severely immunocompromised (transplant recipients, advanced HIV)
— Requires same treatment as TE
— Severe chorioretinitis → blindness
— Hydrocephalus → neurodevelopmental delay
— Hearing loss, seizures
— Highest risk: Toxoplasma IgG-positive donor heart → IgG-negative recipient (D+/R−)
— Prophylaxis with TMP-SMX recommended
Board pearl: After starting ART in a patient with TE, clinical worsening may represent IRIS rather than treatment failure — distinguish by timing (usually within first 4–8 weeks of ART).

— Key distinction from malaria: Babesia shows tetrads (Maltese cross), no pigment (hemozoin); different geographic/exposure history
Board pearl: Babesiosis and malaria both cause intraerythrocytic ring forms — look for Maltese cross (Babesia) vs. banana-shaped gametocytes (P. falciparum) on smear.

— Also ring-enhancing lesion(s) in HIV/AIDS, typically CD4 < 50
— Usually single lesion (vs. multiple in TE), periventricular, crosses midline
— EBV PCR positive in CSF; Toxoplasma IgG often negative
— Key distinction: Empiric TE treatment × 2 weeks → no improvement → biopsy → PCNSL likely
— Thallium SPECT or PET: ↑ uptake in lymphoma, ↓ in toxoplasmosis
— JC virus, CD4 < 200, non-enhancing white matter lesions, no mass effect
— No fever; subacute progressive focal deficits
— History of sinusitis, endocarditis, or immunosuppression
— Often single lesion with prominent surrounding edema
Next best step: HIV patient with ring-enhancing brain lesions → check Toxoplasma IgG → if positive, start empiric TE treatment → reassess in 2 weeks.

Chemoprophylaxis for travelers (by region and resistance):
— Atovaquone-proguanil (Malarone): daily, start 1–2 days before, continue 7 days after (shortest post-travel course)
— Doxycycline: daily, start 1–2 days before, continue 4 weeks after
— Mefloquine: weekly, start 2–3 weeks before, continue 4 weeks after
Non-pharmacologic:
Board pearl: Atovaquone-proguanil has the shortest post-travel course (7 days) — preferred for short trips. Doxycycline and mefloquine require 4 weeks post-travel.

Primary prophylaxis in HIV (CD4 < 100 + Toxoplasma IgG positive):
Secondary prophylaxis (after treated TE):
Prevention in pregnancy:
Transplant recipients:
Board pearl: TMP-SMX covers both PCP and Toxoplasma — one drug, two prophylaxis indications in HIV patients.

— Reportable disease in the United States — notify public health authorities
— Pre-travel counseling is a physician responsibility; document chemoprophylaxis discussion and adherence counseling
— Blood bank safety: travelers to endemic areas deferred from blood donation for specified periods to prevent transfusion-transmitted malaria
— Delayed/missed diagnosis is a common medicolegal issue — maintain high index of suspicion in febrile travelers
— Congenital toxoplasmosis: failure to screen or counsel pregnant women about food/cat hygiene in high-risk settings is a patient safety concern
— HIV patients: ensure Toxoplasma IgG is checked at diagnosis of HIV to guide future prophylaxis decisions
— Informed consent for brain biopsy in empiric TE treatment failure — discuss risks vs. diagnostic necessity
— Organ transplant: Toxoplasma serostatus of donor and recipient must be documented; failure to provide prophylaxis in D+/R− is a preventable error
Board pearl: All HIV patients should have Toxoplasma IgG checked at baseline — a negative result essentially rules out reactivation TE later.
Board pearl: Duffy antigen is the receptor for P. vivax — Duffy-negative individuals are naturally resistant.