eduo
visual
Nervous System
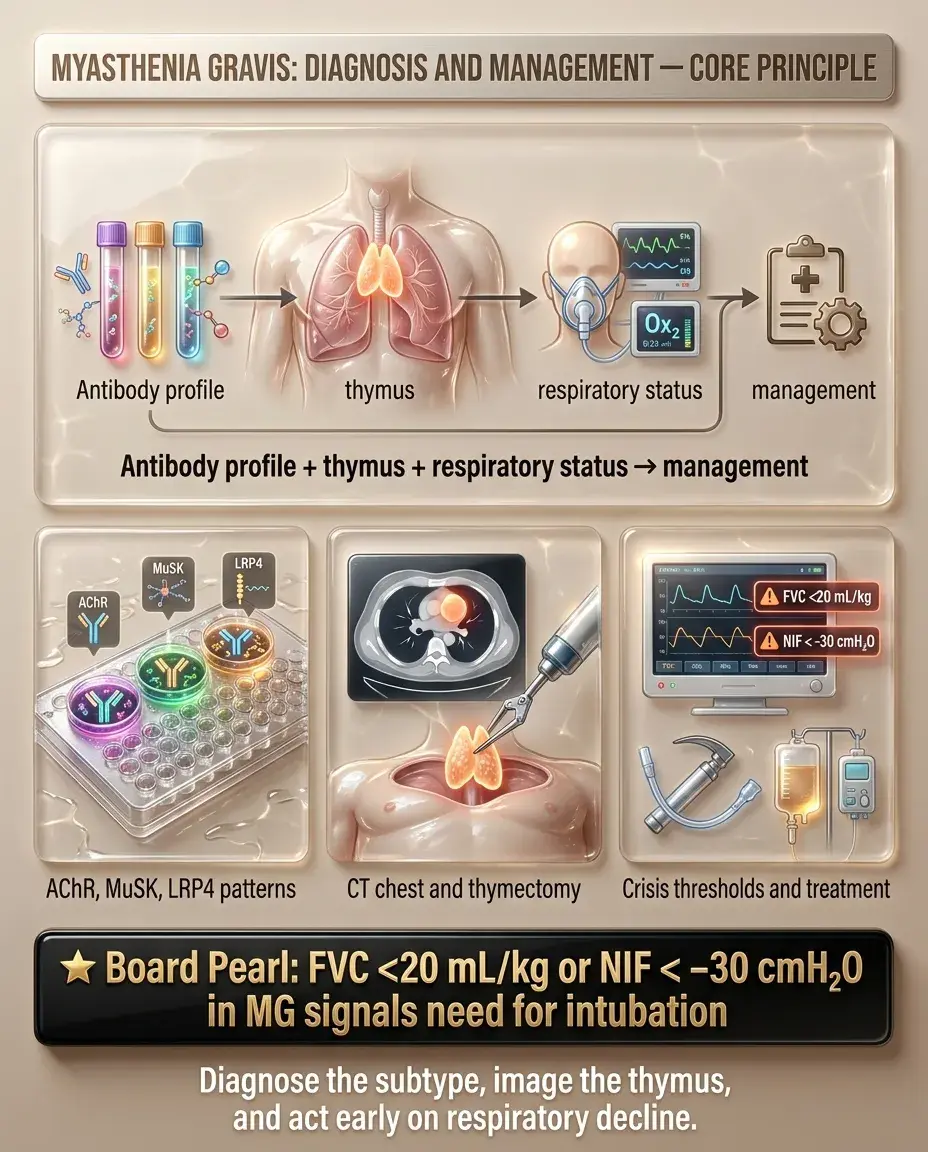
Myasthenia gravis: diagnosis and management
Myasthenia gravis (MG) is an autoimmune disorder caused by antibodies against the postsynaptic neuromuscular junction (NMJ) — most commonly anti-acetylcholine receptor (AChR) antibodies (~85%) → ↓ functional AChR → fatigable weakness.
— Ptosis and diplopia (ocular involvement is the most common initial presentation)
— Difficulty chewing, swallowing, speaking (bulbar weakness)
— Proximal limb weakness
— Symptoms worse at the end of the day
Board pearl: MG affects the postsynaptic NMJ — distinguishing it from Lambert-Eaton (presynaptic) and botulism (presynaptic) is heavily tested.

— Asymmetric ptosis, fluctuating diplopia
— Pupils always spared (unlike CN III palsy from compression)
— Ocular → bulbar → limb/respiratory progression
— Bulbar: dysarthria, dysphagia, nasal voice, jaw fatigue while chewing
— Limb: proximal > distal, arms often > legs
— Respiratory: dyspnea, inability to count to 20 in one breath
Key history clues:
— Symptoms worse with activity, heat, stress, illness, menses
— Associated autoimmune conditions (thyroid disease, RA, SLE)
— Drug-induced exacerbation: aminoglycosides, fluoroquinolones, β-blockers, magnesium, neuromuscular blockers, D-penicillamine
— Thymoma association (10–15%) — ask about chest imaging findings
Next best step: When a patient reports fluctuating diplopia/ptosis with fatigability → test for AChR antibodies.

Important negatives:
— Sensation fully intact
— Reflexes normal
— No fasciculations (distinguishes from ALS)
— Pupils normal
Board pearl: The ice pack test is a safe, noninvasive bedside test for MG-related ptosis — improvement supports diagnosis, especially when edrophonium testing is not readily available.

Step 1 — Antibody testing (most important):
— Highly specific (>99%); positive result essentially confirms diagnosis
— Three types: binding, blocking, modulating — binding is most sensitive
— MuSK-MG: prominent bulbar/facial/respiratory weakness, less ocular
— Often younger women; may have tongue/facial atrophy
— Poor response to AChE inhibitors; responds better to rituximab
Step 2 — Confirm with electrophysiology if antibodies negative:
Board pearl: AChR antibodies are the first-line diagnostic test. A positive result in the right clinical context is diagnostic — no further NMJ testing needed.

Repetitive nerve stimulation (RNS):
Single-fiber EMG (SFEMG):
CT chest (all MG patients):
Key distinction: Edrophonium (Tensilon) test is rarely used now due to cardiac risks (bradycardia) and availability of better diagnostics — antibody testing + EMG have replaced it.

Acetylcholinesterase (AChE) inhibitors — first-line symptomatic treatment:
— Inhibits AChE → ↑ ACh at NMJ → improved neuromuscular transmission
— Onset 30 min, duration 3–4 hours
— May suffice as sole therapy in mild/ocular MG
Side effects (cholinergic):
— Muscarinic: diarrhea, abdominal cramps, ↑ salivation, bradycardia, miosis
— Nicotinic (overdose): fasciculations, weakness — can mimic worsening MG (cholinergic crisis)
— Add glycopyrrolate for muscarinic side effects if needed
Important: Pyridostigmine does NOT alter disease course — it is purely symptomatic. Most patients with generalized MG will need immunotherapy.
Board pearl: MuSK-MG responds poorly to pyridostigmine; consider rituximab early in MuSK-positive disease.

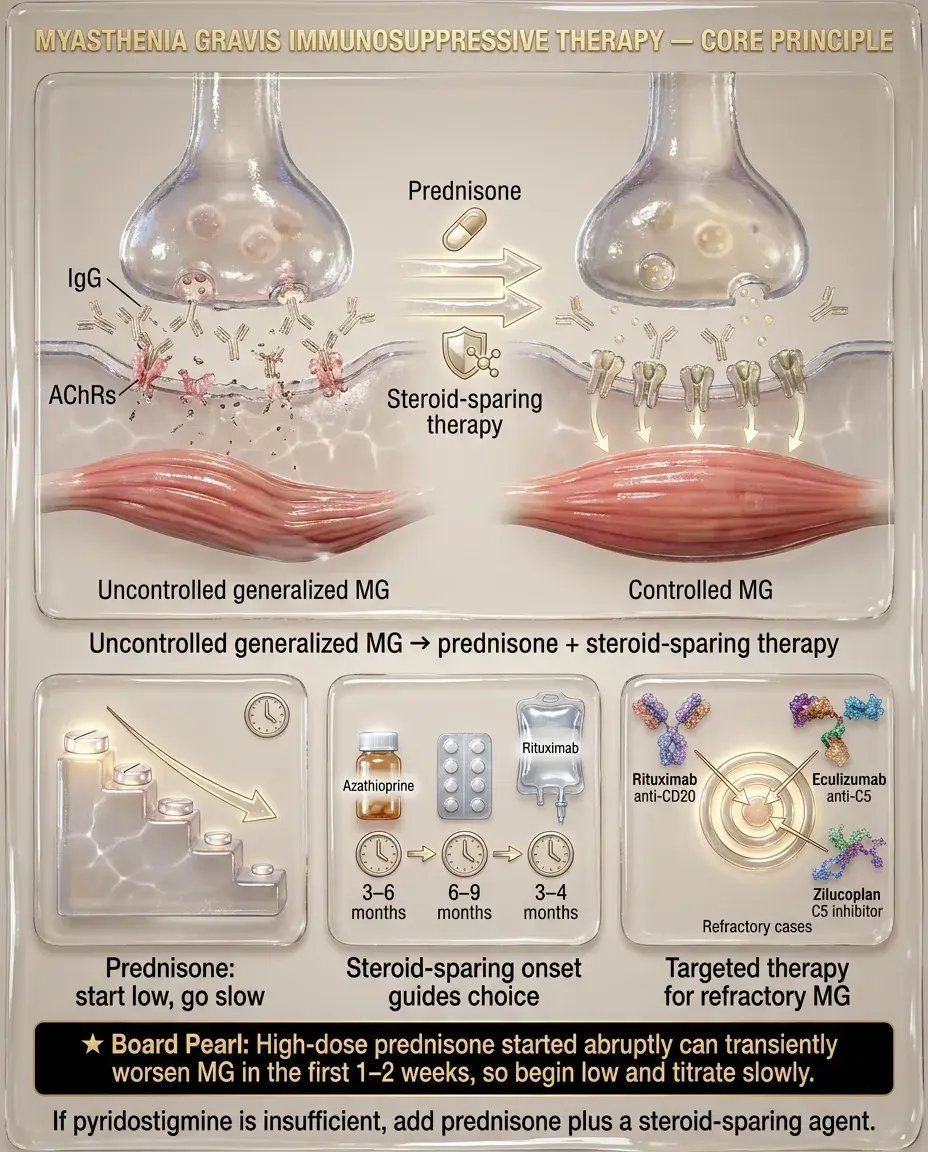
Corticosteroids — first-line immunotherapy for moderate-severe MG:
— Rapid initiation at high dose can paradoxically worsen weakness in first 1–2 weeks ("steroid dip") → start low, go slow, or initiate in-hospital for severe disease
— Once stable, taper to lowest effective dose
Steroid-sparing agents (used with or instead of steroids):
Newer targeted therapy:
Next best step: Generalized MG not controlled by pyridostigmine → add prednisone + steroid-sparing agent.
Thymectomy indications:
Not recommended:
Timing and approach:
Board pearl: Even without thymoma, thymectomy improves outcomes in AChR-Ab+ generalized MG — this is a key Step 2 CK concept from the landmark MGTX randomized trial.

Pregnancy:
Pediatric MG:
— Suspect if onset at birth, family history, seronegative
Board pearl: Never give magnesium sulfate to a pregnant patient with MG — it can precipitate myasthenic crisis.

Elderly-onset MG (>60 years):
Renal impairment:
Hepatic impairment:
Drug interactions — medications that worsen MG:
Next best step: Review medication list in every MG patient — drug-induced exacerbation is a preventable trigger.

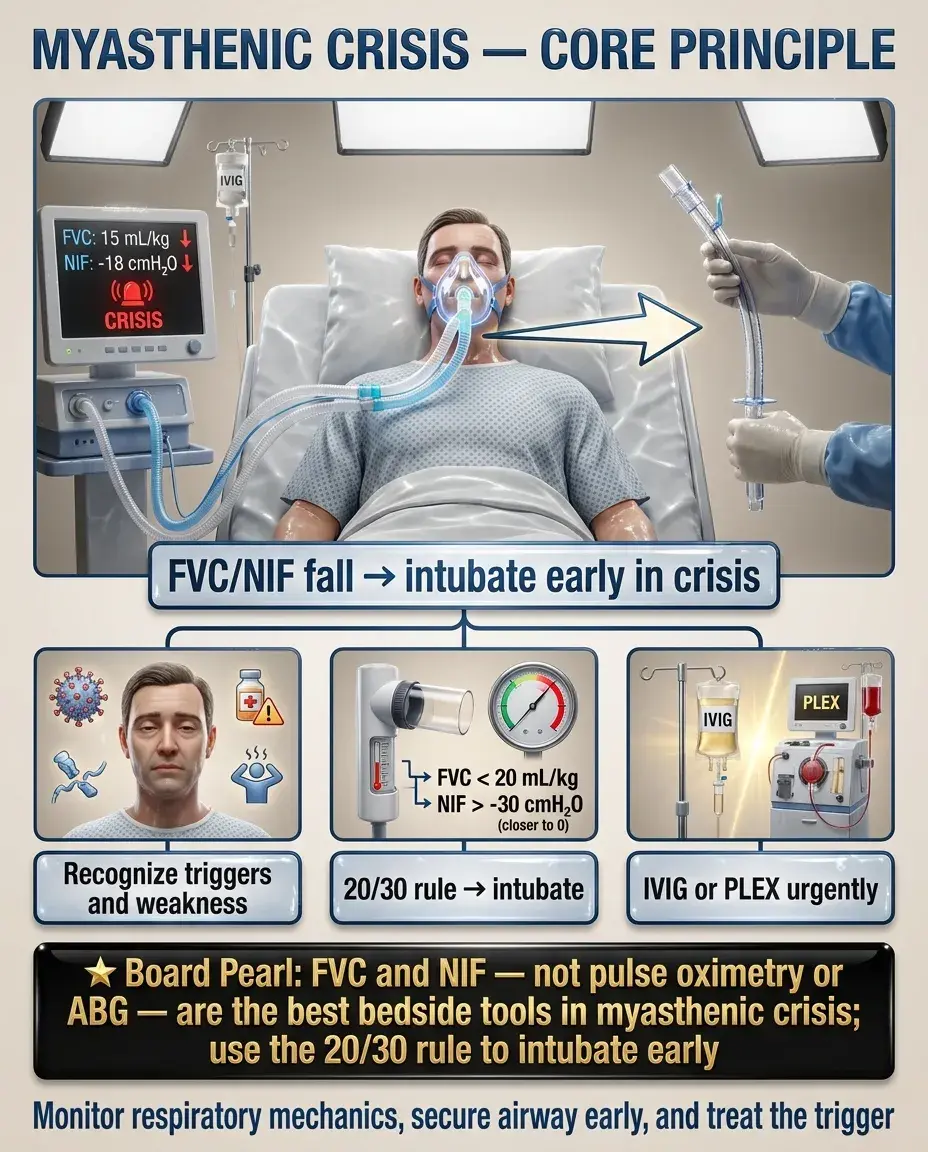
Myasthenic crisis: life-threatening exacerbation with respiratory failure requiring mechanical ventilation — occurs in ~15–20% of MG patients.
— FVC <20 mL/kg or NIF weaker than −30 cmH₂O → intubate (do not wait for ABG deterioration)
Acute treatment:
— Equally effective; IVIG preferred if IV access is difficult
— PLEX faster onset (days); IVIG easier to administer
Board pearl: FVC and NIF — not pulse oximetry or ABG — are the best bedside tools to monitor respiratory function in MG crisis. The "20/30 rule": FVC <20 mL/kg or NIF weaker than −30 cmH₂O → intubate.
Key distinction tested on boards:
— Pupils normal, dry secretions or normal
— Treatment: IVIG/PLEX + ventilatory support
— SLUDGE signs: Salivation, Lacrimation, Urination, Diarrhea, GI cramping, Emesis
— Bradycardia, miosis, fasciculations, excessive bronchial secretions
— Treatment: stop pyridostigmine, atropine for muscarinic effects, ventilatory support
Both present with worsening weakness — differentiation:
— Muscarinic excess → cholinergic crisis
— No muscarinic signs → myasthenic crisis
Board pearl: In a weak MG patient on pyridostigmine with excessive secretions and bradycardia → cholinergic crisis → stop pyridostigmine, give atropine.

Key distinction: Fatigable weakness + pupil-sparing + no sensory loss → think MG. Fixed deficits, pupil involvement, or sensory findings → alternative diagnosis.

— Presynaptic (anti-VGCC antibodies) vs MG (postsynaptic)
— Proximal weakness that IMPROVES with repeated use (opposite of MG)
— Autonomic dysfunction: dry mouth, constipation, erectile dysfunction
— Associated with small cell lung cancer (~60%)
— RNS: incremental response at high frequency (opposite of MG's decremental)
Board pearl: LEMS improves with activity, MG worsens — this distinction is a classic board differentiator. Always screen LEMS patients for small cell lung cancer.

Monitoring on immunotherapy:
Vaccinations:
Board pearl: Before starting eculizumab, meningococcal vaccine is mandatory — unvaccinated patients on complement inhibitors are at high risk for fatal meningococcemia.

Follow-up structure:
Prognosis and natural history:
Poor prognostic indicators:
Board pearl: If purely ocular MG for >2 years without generalization, the likelihood of converting to generalized MG becomes low — an important counseling point.

Driving and occupational safety:
Informed consent for thymectomy:
Perioperative safety:
Medication safety:
Board pearl: Non-depolarizing neuromuscular blockers can cause prolonged paralysis in MG patients — critical anesthesia consideration.