
eduo
visual
Renal & Urinary
Lupus nephritis
Lupus nephritis (LN) → immune complex–mediated glomerulonephritis occurring in ~50% of patients with systemic lupus erythematosus (SLE) → deposition of anti-dsDNA antibodies and complement in the glomeruli → inflammation, proliferation, and/or sclerosis.
— Active urine sediment: proteinuria (often nephrotic range), hematuria, RBC casts
— Rising creatinine or ↓ GFR in an SLE patient
— New-onset HTN or edema in setting of SLE
— Serologic flare: ↑ anti-dsDNA titers + ↓ C3/C4
Board pearl: LN is the most common severe organ manifestation of SLE and the leading cause of morbidity/mortality — every SLE patient needs routine urinalysis and serum creatinine screening at every visit.

— Foamy urine (proteinuria), tea-colored or cola-colored urine (hematuria)
— Peripheral edema, periorbital puffiness (nephrotic syndrome)
— Hypertension — new or worsening
— Fatigue, weight gain from fluid retention
History clues:
— Known SLE with recent flare (rash, arthritis, serositis)
— Non-adherence to hydroxychloroquine (HCQ) — ↑ flare risk
— Medication changes: recent NSAID use may unmask renal dysfunction
— Prior LN episodes — recurrence is common
— Family history of SLE or autoimmune disease
— Pregnancy — LN flares are more common, especially in 2nd/3rd trimester and postpartum
Next best step: In any SLE patient with proteinuria >0.5 g/day, active sediment, or unexplained ↑ Cr → proceed to renal biopsy.

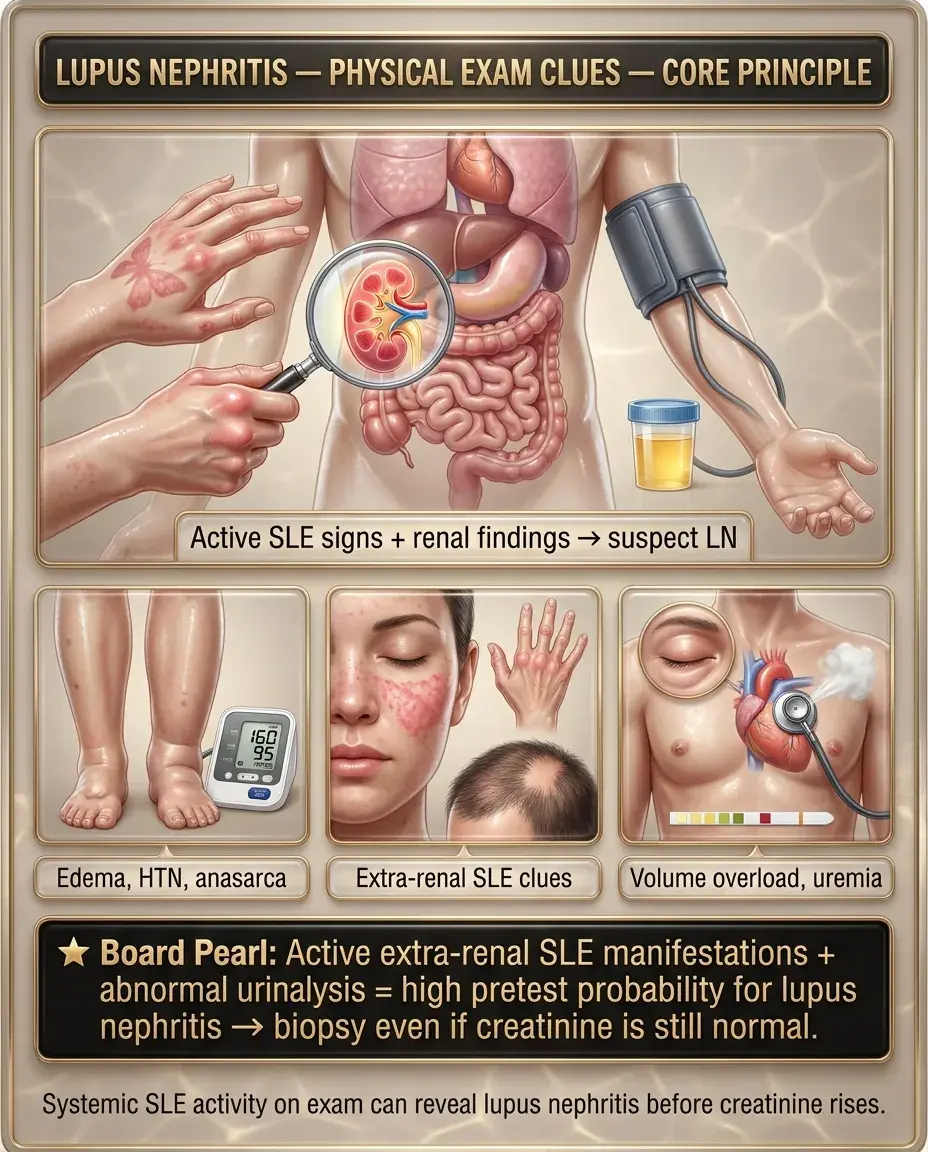
Physical exam often reflects both renal involvement and extra-renal SLE activity:
— Peripheral pitting edema (nephrotic syndrome)
— HTN — often new onset
— Anasarca in severe nephrotic presentations
— Malar (butterfly) rash, discoid lesions
— Oral/nasal ulcers (often painless)
— Arthritis — symmetric, non-erosive
— Alopecia — diffuse, non-scarring
— Serositis — pleural or pericardial rub
— Livedo reticularis (consider antiphospholipid syndrome overlap)
— Volume overload with pulmonary crackles
— Uremic features if progression to ESRD (pericardial rub, asterixis, nausea)
Board pearl: Active extra-renal SLE manifestations + abnormal urinalysis = high pretest probability for LN → biopsy even if creatinine is still normal.
Initial labs:
Serologic markers:
Key distinction: ↑ anti-dsDNA + ↓ C3/C4 = serologic flare → correlates with active nephritis; persistently normal complements make active LN less likely.

Renal biopsy → mandatory for confirmed or suspected LN to guide therapy.
ISN/RPS Classification (2003, updated 2018):
Biopsy also reports activity index (reversible inflammation) vs chronicity index (irreversible scarring).
Board pearl: Class IV is the highest-yield class — most common, most aggressive, and requires the most intensive induction therapy. Always biopsy before starting treatment.

Goal: rapidly suppress active inflammation to preserve nephron mass.
For Class III/IV (± V) LN — aggressive induction:
— Preferred in most patients, especially African American/Hispanic (better response, fewer side effects than cyclophosphamide)
— Reserved for severe proliferative disease, rapidly progressive GN, or MMF failure
For pure Class V (membranous) LN:
Next best step: All LN patients should also receive hydroxychloroquine — ↓ flare risk, ↓ renal progression, ↓ thrombotic events, ↓ mortality.

After 6 months of induction → transition to maintenance (minimum 3–5 years, often longer):
Emerging / adjunctive agents:
Board pearl: Belimumab + standard of care is now a guideline-endorsed strategy for active LN — know this as a tested new addition to the treatment algorithm.

Critical non-immunosuppressive therapies:
— ↓ intraglomerular pressure, ↓ proteinuria, renoprotective
— Target BP <130/80 mmHg
Next best step: Start ACEi/ARB + HCQ in every LN patient regardless of ISN/RPS class.

LN and pregnancy:
— Safe in pregnancy: HCQ (continue — ↓ flare risk), azathioprine, low-dose prednisone, tacrolimus
— Contraindicated: MMF (teratogenic — neural tube defects, cleft lip), cyclophosphamide (teratogenic), ACEi/ARBs (fetotoxic — renal agenesis, oligohydramnios), methotrexate
— Switch MMF → azathioprine ≥3 months before conception
— Switch ACEi/ARB → nifedipine or labetalol for BP control
— LN flare: active sediment, ↑ anti-dsDNA, ↓ complement, extra-renal SLE activity
— Preeclampsia: ↑ LFTs, ↓ platelets, ↑ uric acid, normal/stable complements
Key distinction: ↓ C3/C4 + active sediment + ↑ anti-dsDNA → LN flare; ↑ uric acid + ↑ LFTs + ↓ platelets → preeclampsia.

Pediatric LN:
Elderly patients:
Patients with pre-existing CKD:
Board pearl: In pediatric SLE, biopsy early — disease is more aggressive, and early treatment preserves long-term renal function.

— Creatinine doubling over days to weeks, active sediment, crescents on biopsy
— Escalate: IV pulse methylprednisolone + IV cyclophosphamide ± plasmapheresis
— Consider ICU admission if concurrent pulmonary hemorrhage (lupus pneumonitis/DAH)
— Thromboembolism (renal vein thrombosis, PE) — albumin <2.5 g/dL → prophylactic anticoagulation
— Severe hyperlipidemia → statin therapy
— Infection risk compounded by immunosuppression + urinary Ig losses
— Failure to respond after 6 months of induction → repeat biopsy to reassess class and activity/chronicity
— Switch therapy: MMF failure → CYC (or vice versa)
— Add rituximab or voclosporin
— ~10–20% of LN patients despite therapy
— Prepare for dialysis or transplantation — LN patients do well post-transplant
— Disease quiescence usually required for ≥6 months before transplant listing
Next best step: Refractory LN after 6 months → repeat renal biopsy before changing therapy.

— ~30–40% of SLE patients have antiphospholipid antibodies
— APS nephropathy: thrombotic microangiopathy (TMA) on biopsy → arteriolar thrombosis, fibrin thrombi, cortical ischemia
— Distinct from immune complex LN — may coexist
— Treatment: anticoagulation (warfarin, target INR 2–3); immunosuppression alone insufficient
— SLE patients at ↑ risk for TTP/HUS
— Microangiopathic hemolytic anemia (schistocytes), thrombocytopenia, renal failure, fever, neurologic changes
— Urgent: ADAMTS13 activity, peripheral smear → plasma exchange if TTP suspected
Key distinction: LN = immune complex GN (active sediment, low complement) vs APS nephropathy = thrombotic process (TMA on biopsy, positive aPL) vs TTP = MAHA + thrombocytopenia + ADAMTS13 <10%.

Not all renal disease in SLE is lupus nephritis:
— NSAIDs → acute interstitial nephritis (AIN) or hemodynamic AKI
— Calcineurin inhibitors (tacrolimus) → ↑ Cr from vasoconstriction
— Look for eosinophiluria (AIN), recent med changes
Board pearl: Always biopsy to confirm LN rather than empirically treating — the differential is broad, and management differs dramatically based on histologic class.

— LN Class V: "full house" immunofluorescence (IgG, IgA, IgM, C3, C1q) + subepithelial deposits
— Primary MN: IgG4-dominant, anti-PLA2R antibodies positive in ~70–80%, no C1q
— Key distinction: C1q positivity + "full house" IF = lupus membranous
— FSGS: podocyte injury, segmental sclerosis, no immune deposits
— LN can have secondary FSGS-like changes in chronic disease
— Foot process effacement on EM without immune deposits
— Check ANCA if biopsy shows crescents without immune deposits
Next best step: "Full house" immunofluorescence on biopsy is virtually pathognomonic for lupus nephritis.

Active disease monitoring (during induction):
Remission monitoring (during maintenance):
Response definitions:
Board pearl: Serologic flare (↑ anti-dsDNA, ↓ C3/C4) may precede clinical flare by weeks — use as an early warning to intensify monitoring.

— ↓ renal flare rate by ~50%
— ↓ damage accrual, ↓ thrombosis, ↓ mortality
— Never discontinue unless retinal toxicity develops
— Chronic steroids → infection, osteoporosis, AVN, metabolic syndrome
Long-term outcomes:
Board pearl: Persistent proteinuria at 12 months (UPCR >0.7–1.0) predicts long-term renal decline — intensify therapy if remission targets are not met.

— Cyclophosphamide is gonadotoxic → discuss oocyte/sperm cryopreservation before treatment, especially in young patients
— GnRH agonists (leuprolide) may be co-administered with CYC to ↓ ovarian failure risk
— MMF is teratogenic — ensure reliable contraception + pregnancy testing before initiation
— Risks: bleeding (most common), perinephric hematoma, AV fistula, infection
— Benefit: guides therapy and avoids empiric immunosuppression
— Biopsy is standard of care — declining biopsy limits ability to treat optimally
— Non-adherence is the leading modifiable risk factor for LN flare and ESRD
— Address barriers: cost (MMF vs generic), complexity, side effects, health literacy
— Involve social work, pharmacy, patient navigators in high-risk populations
— African American, Hispanic, and Asian patients have worse LN outcomes — partly biologic, partly due to social determinants of health
— Equitable access to nephrology, rheumatology, and newer agents (belimumab, voclosporin) must be addressed
Board pearl: Always counsel on fertility preservation before cyclophosphamide — this is a testable patient safety issue.

Board pearl: Wire-loop lesions = subendothelial immune deposits so thick they resemble capillary wall thickening on LM → Class IV LN.


