eduo
visual
Infectious Disease
Histoplasmosis, coccidioidomycosis, blastomycosis
Three dimorphic fungi cause most endemic mycoses in North America:
All exist as mold in soil (25°C) → convert to yeast at body temp (37°C) — except Coccidioides → spherules
Suspect endemic mycosis when:
Board pearl: Geography is the #1 clue — always note the patient's state of residence or travel history.

— Often self-limited in immunocompetent hosts
— CXR: diffuse reticulonodular infiltrates, hilar/mediastinal lymphadenopathy
— Fever, weight loss, hepatosplenomegaly, pancytopenia
— Skin: papules, nodules, oral ulcers
— Adrenal involvement → adrenal insufficiency
Board pearl: Histo + pancytopenia + hepatosplenomegaly in AIDS → think disseminated histoplasmosis.

Coccidioidomycosis (Valley fever):
Blastomycosis:
Key distinction: Verrucous skin lesions → blasto; erythema nodosum → cocci; oral ulcers + pancytopenia → histo.

— Cross-reacts with Blastomyces
— CSF CF antibody confirms cocci meningitis
Next best step for suspected endemic mycosis:
Board pearl: Cocci CF titer ≥1:32 → high risk of dissemination.

Culture (gold standard for all three):
Histopathology:
Imaging:
Board pearl: Broad-based budding = Blasto; intracellular yeast = Histo; spherules with endospores = Cocci.

Mild/moderate pulmonary disease:
Key distinction: Blasto is the only one where mild disease always requires treatment — spontaneous resolution is unreliable.
Itraconazole dosing:
Board pearl: Itraconazole is the azole of choice for mild-moderate histo and blasto; fluconazole is preferred for cocci.

Severe pulmonary or disseminated disease (all three fungi):
— Histo: itraconazole × ≥12 months
— Cocci: fluconazole (or itraconazole) × ≥12 months
— Blasto: itraconazole × ≥12 months
Coccidioidal meningitis:
Next best step: Severe disease with hypoxia or hemodynamic instability → start amphotericin B immediately, then de-escalate to azole once clinically stable.

Histo in HIV/AIDS (CD4 < 150):
Cocci in HIV/AIDS:
De-escalation principles:
Board pearl: Cocci meningitis requires lifelong fluconazole — never discontinue even if HIV is well controlled.

Coccidioidomycosis in pregnancy:
Histoplasmosis/blastomycosis in pregnancy:
Board pearl: Pregnant woman from Arizona with pneumonia + erythema nodosum → suspect cocci → treat with amphotericin B, NOT fluconazole.

Pediatric:
Immunosuppressed (transplant, anti-TNF):
Renal impairment:
Board pearl: Always check azole–immunosuppressant interactions in transplant patients.
Histoplasmosis complications:
Coccidioidomycosis complications:
Blastomycosis complications:
When to escalate:
Board pearl: Fibrosing mediastinitis is a late, irreversible complication of histo — NOT an indication for antifungals.

Immune reconstitution inflammatory syndrome (IRIS):
Management of IRIS:
Next best step: Worsening symptoms after ART initiation with falling Histoplasma antigen → IRIS → supportive care ± corticosteroids.

Endemic mycosis vs TB:
Endemic mycosis vs sarcoidosis:
Blasto vs lung cancer:
Board pearl: Young patient from Ohio Valley with bilateral hilar LAD → rule out histo before diagnosing sarcoidosis.

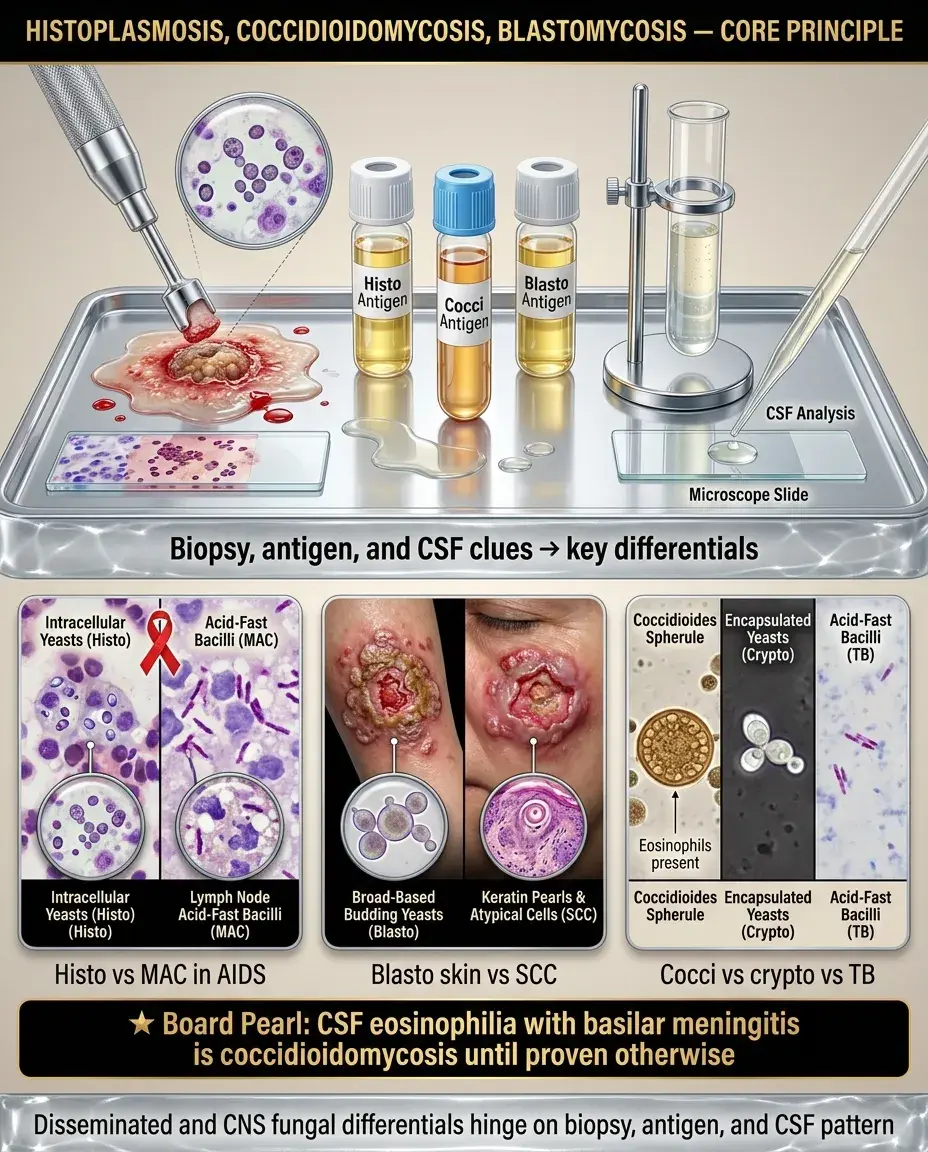
Disseminated histo vs disseminated MAC in AIDS:
Blasto skin vs squamous cell carcinoma:
Cocci meningitis vs TB meningitis vs cryptococcal:
Key distinction: CSF eosinophilia + basilar meningitis = cocci until proven otherwise.
Primary prophylaxis:
Secondary prophylaxis (after treatment of active disease in HIV):
Pre-transplant screening:
Board pearl: Secondary prophylaxis is more commonly tested than primary prophylaxis for endemic mycoses.

Itraconazole monitoring:
Response assessment:
Duration:
Next best step: Patient on itraconazole with rising Histoplasma antigen → assess adherence, check drug levels, consider switch to amphotericin B.

— Employers should provide respiratory protection in endemic zones
Patient counseling:
Board pearl: Always notify the lab when sending samples for suspected dimorphic fungi — accidental lab exposure is a real safety risk.