top of page

eduo
visual
Microbiology
Gram-Positive Rods: Bacillus, Clostridium (tetani, botulinum, perfringens, difficile), Corynebacterium, Listeria
Core Principle of Gram-Positive Rods
Gram-positive rods are a heterogeneous group of bacteria united by their rod shape and thick peptidoglycan cell wall that retains crystal violet stain.
Key genera include spore-formers (Bacillus, Clostridium), non-spore-formers (Corynebacterium, Listeria), and each has distinct pathogenic mechanisms.
Spore formation allows survival in harsh environments — a critical virulence factor for Bacillus and Clostridium species.
Board pearl: Spore-forming gram-positive rods are either aerobic (Bacillus) or anaerobic (Clostridium) — this oxygen requirement is the primary distinguishing feature between these genera.

Bacillus anthracis: The Anthrax Agent
B. anthracis forms centrally located spores that do not cause swelling of the bacterial cell — appears as "boxcar-shaped" rods in chains.
Virulence depends on a poly-D-glutamate capsule (unique among bacteria — not polysaccharide) and two toxins: edema factor (EF) and lethal factor (LF).
Three clinical forms: cutaneous (95% of cases) → painless black eschar; pulmonary → widened mediastinum on CXR; gastrointestinal → rare but high mortality.
Board pearl: Woolsorter's disease = inhalation anthrax from contaminated animal hides; presents with flu-like symptoms → rapid progression to hemorrhagic mediastinitis.

Bacillus cereus: Food Poisoning Syndromes
B. cereus causes two distinct food poisoning syndromes based on different toxins and incubation periods.
Emetic syndrome: preformed cereulide toxin in reheated rice → rapid onset (1-6 hours) of nausea and vomiting, self-limited.
Diarrheal syndrome: heat-labile enterotoxin produced in vivo → longer incubation (8-16 hours), watery diarrhea.
Also causes serious infections in immunocompromised patients: bacteremia, endophthalmitis (especially post-traumatic), pneumonia.
Board distinction: Short incubation + vomiting + rice = B. cereus emetic form; longer incubation + diarrhea = diarrheal form.

Clostridium tetani: Tetanus Pathogenesis
C. tetani produces tetanospasmin, a neurotoxin that blocks release of inhibitory neurotransmitters (GABA and glycine) from Renshaw cells in the spinal cord.
Loss of inhibition → unopposed muscle contraction → spastic paralysis (contrast with botulism's flaccid paralysis).
Clinical features: trismus (lockjaw), risus sardonicus (grimace), opisthotonus (arched back), autonomic instability.
Spores ubiquitous in soil; enter through wounds (especially puncture wounds, burns, injection drug use).
Board pearl: Tetanus toxin travels retrograde up motor neurons to reach the spinal cord — this explains why symptoms often begin near the wound site.

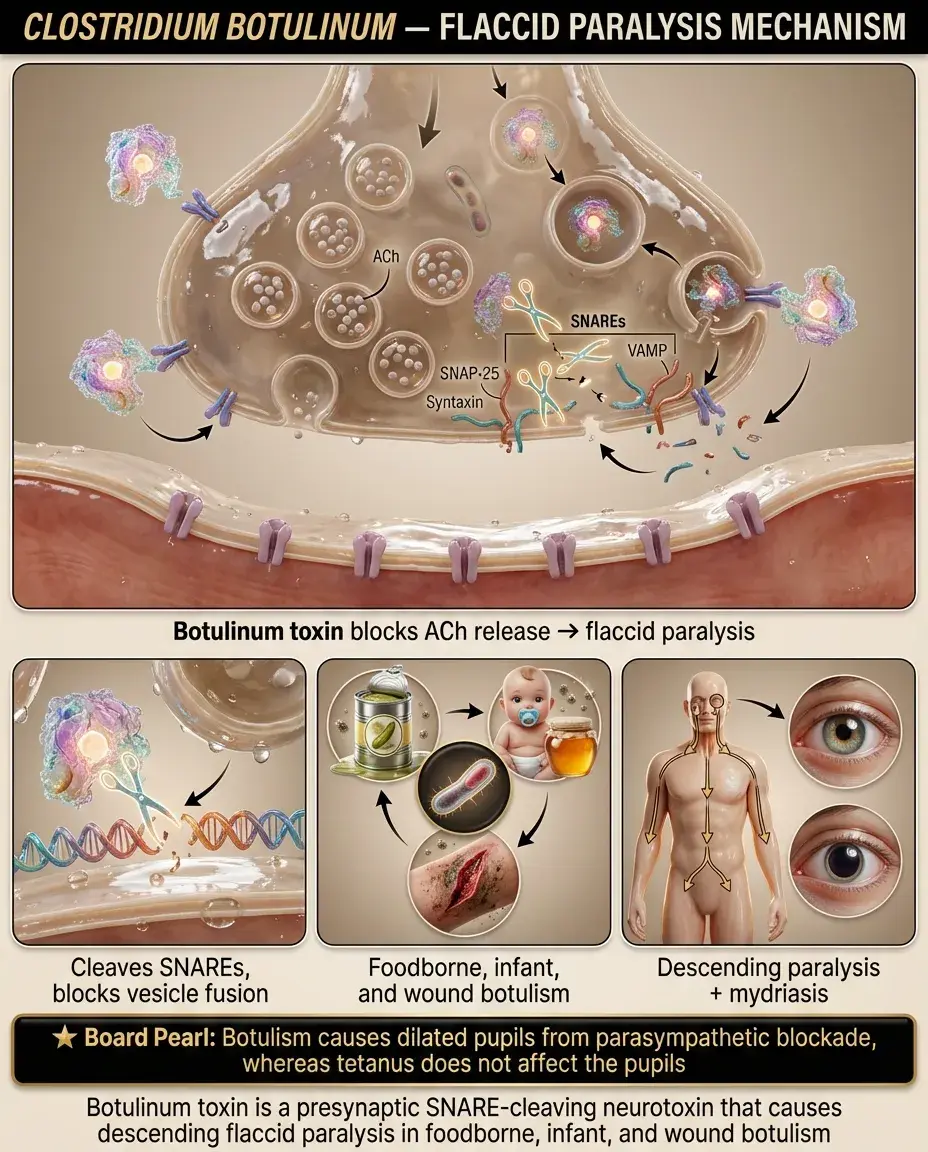
Clostridium botulinum: Mechanism of Flaccid Paralysis
Botulinum toxin cleaves SNARE proteins (SNAP-25, synaptobrevin) → prevents acetylcholine release at neuromuscular junctions → flaccid paralysis.
Adult botulism: preformed toxin in canned/preserved foods → descending paralysis starting with cranial nerves (diplopia, dysphagia, dysarthria).
Infant botulism: spore ingestion (honey exposure) → in vivo toxin production → floppy baby syndrome.
Wound botulism: increasingly common in injection drug users, especially black tar heroin.
Board pearl: Botulism causes mydriasis (dilated pupils) due to parasympathetic blockade; tetanus does not affect pupils.
Clostridium perfringens: Gas Gangrene and Food Poisoning
C. perfringens produces alpha toxin (lecithinase/phospholipase C) → destroys cell membranes → myonecrosis and hemolysis.
Gas gangrene: traumatic wounds → rapid tissue destruction, gas in tissues (crepitus), bronze skin discoloration, septic shock.
Food poisoning: heat-resistant spores survive cooking → germinate during cooling → enterotoxin production in the intestine → watery diarrhea 8-16 hours after ingestion.
Board distinction: Gas gangrene has rapid onset (<24 hours) with severe pain out of proportion to exam findings; food poisoning is self-limited without fever.

Clostridium difficile: Antibiotic-Associated Colitis
C. difficile produces two toxins: Toxin A (enterotoxin) attracts neutrophils; Toxin B (cytotoxin) causes cell death — both contribute to pseudomembrane formation.
Risk factors: antibiotic use (especially clindamycin, fluoroquinolones, cephalosporins), hospitalization, age >65, PPI use.
Spectrum: asymptomatic carriage → mild diarrhea → fulminant colitis with toxic megacolon.
Diagnosis: PCR or enzyme immunoassay for toxin; colonoscopy shows yellow-white pseudomembranes.
Board pearl: C. difficile is the most common cause of antibiotic-associated diarrhea and nosocomial diarrhea.

Corynebacterium diphtheriae: Exotoxin-Mediated Disease
C. diphtheriae produces diphtheria toxin only when infected by lysogenic bacteriophage carrying the tox gene.
Toxin mechanism: ADP-ribosylates elongation factor-2 (EF-2) → halts protein synthesis → cell death.
Local effects: grayish pseudomembrane in pharynx that bleeds when scraped; can cause airway obstruction.
Systemic effects: myocarditis (most common cause of death), peripheral neuropathy, renal tubular necrosis.
Laboratory: club-shaped rods in "Chinese letter" arrangement; grow on tellurite agar (black colonies) and Loeffler medium.
Board pearl: Bull neck appearance = massive cervical lymphadenopathy in severe diphtheria.

Listeria monocytogenes: Intracellular Pathogen
L. monocytogenes uses internalin proteins to invade intestinal epithelium, then escapes the phagosome using listeriolysin O.
Unique motility: actin polymerization creates "rocket tails" allowing cell-to-cell spread without extracellular exposure.
Grows at refrigerator temperatures (4°C) — contaminated deli meats, soft cheeses, unpasteurized dairy are common sources.
At-risk populations: pregnant women (can cross placenta → spontaneous abortion, neonatal sepsis), elderly, immunocompromised.
Board pearl: Listeria is the third most common cause of neonatal meningitis and the most common cause of meningitis in adults >60 years old.

Laboratory Identification of Gram-Positive Rods
Bacillus: large, aerobic, spore-forming; B. anthracis is non-motile and non-hemolytic (unique among Bacillus species).
Clostridium: anaerobic, spore-forming; location of spore (terminal vs. subterminal) helps with species identification.
Corynebacterium: non-spore-forming, catalase-positive, club-shaped with metachromatic granules (volutin).
Listeria: non-spore-forming, catalase-positive, tumbling motility at room temperature, β-hemolytic on blood agar.
Board clue: Gram-positive rods + anaerobic = Clostridium; + aerobic spores = Bacillus; + tumbling motility = Listeria.

Toxin Mechanisms and Clinical Correlations
Neurotoxins: tetanospasmin blocks inhibitory neurons → spastic paralysis; botulinum blocks ACh release → flaccid paralysis.
Cytotoxins: diphtheria toxin inhibits protein synthesis; C. difficile toxins A/B disrupt cytoskeleton; alpha toxin destroys membranes.
Enterotoxins: B. cereus and C. perfringens cause food poisoning through different mechanisms but similar presentations.
Board distinction: Spastic paralysis = tetanus; flaccid paralysis = botulism; pseudomembrane in throat = diphtheria; pseudomembrane in colon = C. difficile.

Special Clinical Scenarios and Risk Factors
Neonatal tetanus: umbilical stump contamination in unvaccinated mothers → generalized rigidity, poor feeding, opisthotonus.
Infant botulism: honey exposure in infants <12 months → constipation, weak cry, loss of head control, eventual respiratory failure.
Listeriosis in pregnancy: flu-like illness in mother → devastating fetal effects (granulomatosis infantiseptica).
Gas gangrene: deep puncture wounds, compound fractures, retained foreign bodies → rapid progression requiring emergent debridement.
Board pearl: Any gram-positive rod in CSF of a neonate should raise suspicion for Listeria.

Pathologic Findings and Tissue Manifestations
Anthrax: hemorrhagic mediastinitis with widened mediastinum; cutaneous lesions show coagulation necrosis.
Gas gangrene: muscle necrosis with gas bubbles in tissue; brick-red, liquefied muscle at surgery.
Diphtheria: fibrinous pseudomembrane composed of fibrin, dead cells, bacteria; firmly adherent.
C. difficile: volcano-like pseudomembranes on colonoscopy; marked neutrophilic infiltration on histology.
Board clue: Pseudomembranes that bleed when removed = diphtheria; yellow-white plaques in colon = C. difficile.

Epidemiology and Transmission Patterns
Anthrax: zoonotic disease from infected animals; bioterrorism concern due to spore stability.
Tetanus: ubiquitous environmental spores; disease reflects vaccination status, not exposure.
Botulism: geographic clustering based on food preservation practices; wound botulism increasing with IV drug use.
C. difficile: nosocomial transmission via spores; alcohol-based sanitizers ineffective — requires soap and water.
Listeria: foodborne outbreaks from contaminated processed foods; vertical transmission during pregnancy.
Board pearl: Only C. difficile spreads person-to-person in healthcare settings via spore transmission.

Prevention Strategies and Prophylaxis
Tetanus: active immunization with toxoid (DTaP series); passive immunization with TIG for high-risk wounds in unvaccinated patients.
Diphtheria: toxoid vaccine prevents disease but not colonization; close contacts need antibiotic prophylaxis.
Anthrax: post-exposure prophylaxis with ciprofloxacin or doxycycline × 60 days due to spore germination risk.
Botulism: proper food canning techniques; avoid honey in infants <12 months.
C. difficile: antimicrobial stewardship, contact precautions, environmental cleaning with sporicidal agents.
Board pearl: Tetanus prophylaxis depends on wound type AND vaccination history — clean wounds need TIG only if <3 lifetime doses.

Treatment Principles and Antitoxins
Tetanus: tetanus immune globulin (TIG) neutralizes unbound toxin; metronidazole for active infection; supportive care in ICU.
Botulism: trivalent antitoxin (A, B, E) for adults; BIG-IV (botulism immune globulin) for infant botulism.
Diphtheria: diphtheria antitoxin (horse serum — test for hypersensitivity first) plus antibiotics (penicillin or erythromycin).
Gas gangrene: emergent surgical debridement + high-dose penicillin G + clindamycin (reduces toxin production).
Board pearl: Antitoxins must be given early — they neutralize only unbound toxin, not toxin already bound to tissues.

Complications and Long-Term Sequelae
Tetanus: autonomic dysfunction (labile blood pressure, arrhythmias), fractures from severe spasms, aspiration pneumonia.
Botulism: prolonged weakness requiring mechanical ventilation; complete recovery possible but may take months.
Diphtheria: myocarditis (2-3 weeks post-infection), polyneuropathy (palatal paralysis → nasal speech), renal failure.
C. difficile: recurrence in 20-30% after first episode; fulminant colitis → perforation, toxic megacolon.
Listeria: meningitis complications include hydrocephalus, brain abscess; high mortality in neonatal disease.
Board clue: Palatal paralysis with nasal speech weeks after pharyngitis = post-diphtheritic polyneuropathy.

Diagnostic Pitfalls and Differential Considerations
Tetanus: no laboratory test confirms diagnosis — purely clinical based on symptoms + exposure history.
Infant botulism: often misdiagnosed as sepsis, dehydration, or failure to thrive — consider in any floppy infant.
Gas gangrene vs. necrotizing fasciitis: both have rapid progression but gas gangrene involves muscle, fasciitis spares muscle.
C. difficile: can cause disease even 2-3 months after antibiotic exposure; consider in any nosocomial diarrhea.
Listeria meningitis: may have minimal CSF pleocytosis in immunocompromised patients — always culture CSF.
Board pearl: Normal CSF glucose in bacterial meningitis suggests Listeria (partially treated) or viral/TB meningitis.

Board Question Stem Patterns
Boxcar-shaped gram-positive rods + widened mediastinum → Bacillus anthracis (inhalation anthrax).
Reheated rice + rapid vomiting → B. cereus emetic syndrome.
Puncture wound + trismus + opisthotonus → tetanus.
Canned foods + descending paralysis + dilated pupils → botulism.
Recent antibiotics + pseudomembranous colitis → C. difficile.
Deli meats + pregnant woman + meningitis → Listeria.
Pharyngeal pseudomembrane + myocarditis → diphtheria.
Trauma + gas in tissues + brick-red muscle → gas gangrene (C. perfringens).

One-Line Recap
Gram-positive rods encompass spore-formers that survive extreme conditions (aerobic Bacillus causing anthrax; anaerobic Clostridium causing tetanus, botulism, gas gangrene, and C. diff colitis) and non-spore-formers causing toxin-mediated disease (Corynebacterium diphtheriae) or intracellular infections in at-risk populations (Listeria in pregnancy and extremes of age).

bottom of page