top of page

eduo
visual
Add a Title
Add paragraph text. Click “Edit Text” to update the font, size and more. To change and reuse text themes, go to Site Styles.
Core Principle of Erythrocyte Deformability
Erythrocyte deformability is the ability of red blood cells to reversibly change shape without lysing as they traverse capillaries smaller than their 7-8 μm diameter.
This property depends on three key factors: biconcave disc geometry (provides optimal surface-to-volume ratio), membrane elasticity (spectrin-actin cytoskeleton network), and cytoplasmic viscosity (hemoglobin concentration and hydration state).
Deformability allows RBCs to squeeze through 3-4 μm capillaries and splenic sinusoids, deliver oxygen to tissues, and survive 120 days in circulation.
Loss of deformability → premature RBC destruction in the spleen → hemolytic anemia.

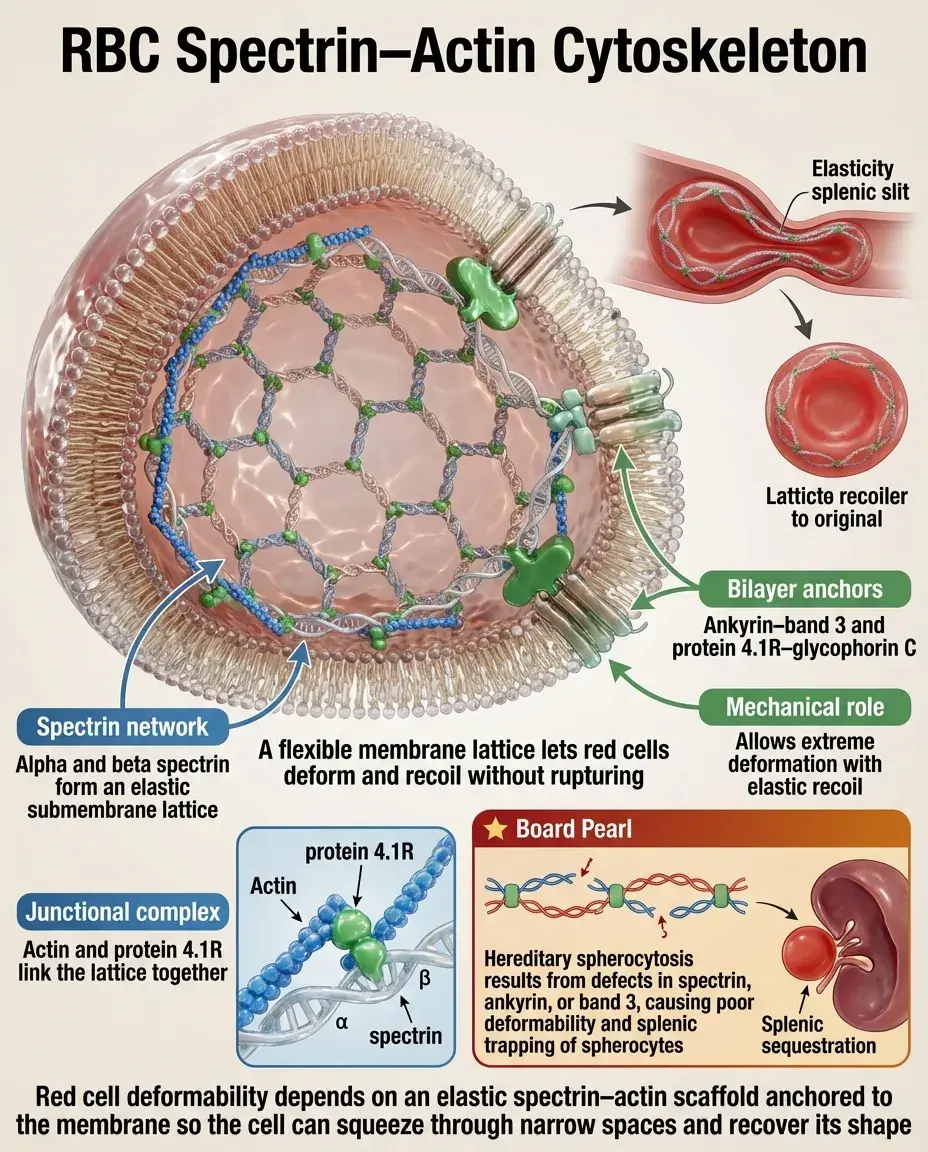
The Spectrin-Actin Cytoskeleton Network
The RBC membrane skeleton consists of α and β spectrin tetramers cross-linked by short actin filaments and protein 4.1R at junctional complexes.
This hexagonal lattice network provides elastic recoil — the membrane can stretch up to 250% of resting length and snap back without damage.
Spectrin connects to the lipid bilayer via two major linkages: ankyrin (links β-spectrin to band 3) and protein 4.1R complex (links to glycophorin C).
Board pearl: Hereditary spherocytosis → spectrin, ankyrin, or band 3 defects → loss of membrane elasticity → spherocytes that cannot deform → splenic trapping.
Surface Area-to-Volume Ratio and the Biconcave Shape
Normal RBCs have 40% more surface area than a sphere of equivalent volume — this excess membrane enables deformation without increasing tension.
The biconcave shape maximizes surface area for gas exchange while minimizing diffusion distance from membrane to center.
Loss of membrane surface area (hereditary spherocytosis) or gain of cell volume (thalassemia) → decreased SA:V ratio → spherical shape → rigid cell.
Board distinction: Spherocytes are uniformly round; target cells have excess membrane creating a central density; both affect deformability differently.

Hemoglobin Concentration and Cytoplasmic Viscosity
Normal mean corpuscular hemoglobin concentration (MCHC) is 32-36 g/dL — precisely regulated to optimize oxygen carrying capacity without compromising deformability.
Increased MCHC → increased cytoplasmic viscosity → decreased deformability. Seen in hereditary spherocytosis (membrane loss concentrates hemoglobin) and xerocytosis.
Decreased MCHC → improved deformability but reduced oxygen capacity. Seen in iron deficiency anemia and thalassemia trait.
Board pearl: Sickle cell disease → HbS polymerization dramatically increases viscosity → rigid, non-deformable cells → vaso-occlusion.

ATP and the Maintenance of Deformability
RBCs require ATP to maintain Na⁺/K⁺-ATPase activity, preserve cell volume, and keep membrane lipids asymmetrically distributed.
ATP depletion → loss of ion gradients → cell swelling → echinocyte formation → irreversibly rigid spheroechinocytes.
Glycolytic enzyme defects (pyruvate kinase deficiency) → ATP depletion → rigid cells → hemolysis particularly in metabolically stressed states.
Storage lesion: banked RBCs progressively lose ATP → decreased deformability → immediate post-transfusion clearance of the most damaged cells.

The Spleen as the Deformability Filter
Splenic sinusoids have 2-3 μm inter-endothelial slits — RBCs must deform extensively to pass from splenic cords to sinuses.
Non-deformable RBCs are retained in the cords → exposed to splenic macrophages → phagocytosed (extravascular hemolysis).
The spleen also "conditions" RBCs by removing excess membrane, creating the normal biconcave shape from reticulocytes.
Board pearl: Splenectomy improves hemolysis in spherocytosis because it removes the site where rigid spherocytes are trapped and destroyed.

Hereditary Spherocytosis: The Prototype Deformability Defect
Autosomal dominant (75%) or recessive defects in spectrin, ankyrin, band 3, or protein 4.2 → vertical membrane instability.
Membrane vesiculation → progressive surface area loss → spherocyte formation → decreased deformability → splenic trapping.
Laboratory findings: spherocytes on smear, increased MCHC, elevated indirect bilirubin, positive osmotic fragility test.
Board distinction: Unlike other hemolytic anemias, the direct antiglobulin test (Coombs) is negative — this is an intrinsic RBC defect.

Sickle Cell Disease and Irreversible Sickling
Deoxygenated HbS polymerizes → long rigid polymers → classic sickle shape → membrane damage → irreversibly sickled cells (ISCs).
ISCs remain rigid even when reoxygenated due to permanent membrane damage and cytoskeletal reorganization.
Rigid sickle cells occlude microvasculature → tissue ischemia → pain crises and organ damage.
Hydroxyurea increases HbF → dilutes HbS → reduces polymerization → improves deformability → fewer crises.

Malaria and RBC Deformability
Plasmodium infection progressively stiffens RBCs through multiple mechanisms: parasite proteins inserted into membrane, knob formation, and altered cytoskeleton.
Infected RBCs lose deformability → splenic clearance → anemia. But P. falciparum-infected cells also cytoadhere to endothelium → sequestration.
Board pearl: Hereditary elliptocytosis and Southeast Asian ovalocytosis provide malaria resistance by making RBCs too rigid for optimal parasite development.
Artemisinin derivatives work partly by further stiffening infected RBCs → enhanced splenic clearance.

Membrane Lipid Abnormalities
Acanthocytes (spur cells): seen in abetalipoproteinemia and severe liver disease. Abnormal membrane cholesterol:phospholipid ratio → rigid spiculated cells.
Target cells: excess membrane relative to volume seen in liver disease, thalassemia, and post-splenectomy. Increased deformability until extreme excess causes rigidity.
Stomatocytes: cup-shaped RBCs from membrane lipid imbalance. Can be hereditary or acquired (alcoholism).
Board pearl: Acanthocytes must be distinguished from echinocytes (artifact) — acanthocytes have irregular projections, echinocytes have uniform small projections.

Oxidative Damage and Deformability
Oxidative stress → membrane lipid peroxidation, spectrin oxidation, and hemoglobin denaturation (Heinz bodies) → rigid cells.
G6PD deficiency → inadequate NADPH → cannot regenerate reduced glutathione → oxidative damage during stress → rigid cells → hemolysis.
Heinz bodies attach to membrane → bite cells (RBCs with membrane bites removed by spleen) → eventually rigid spherocytes.
Board clue: Hemolysis after fava beans, antimalarials, or infection in African American male → G6PD deficiency → oxidative rigidity.

Pyruvate Kinase Deficiency
Most common glycolytic enzyme defect → decreased ATP production → cannot maintain ion pumps → rigid echinocytes.
Autosomal recessive, presents with chronic hemolytic anemia worse during infections or pregnancy (increased metabolic demand).
Post-splenectomy paradoxical improvement in hemoglobin despite persistent enzyme defect — removes site of destruction.
Board distinction: Unlike G6PD deficiency (episodic hemolysis), PK deficiency causes chronic hemolysis with echinocytes rather than bite cells.

Microangiopathic Hemolytic Anemia
RBC fragmentation occurs when cells are forced through fibrin strands in microvasculature → schistocytes (helmet cells, triangle cells).
Common causes: TTP, HUS, DIC, malignant hypertension, mechanical heart valves, march hemoglobinuria.
Fragmented cells have lost membrane → spherocytic fragments with poor deformability → rapid splenic clearance.
Board pearl: Schistocytes + thrombocytopenia + neurologic symptoms → TTP. Schistocytes + thrombocytopenia + renal failure → HUS.

Temperature Effects on Deformability
Cold agglutinin disease: IgM antibodies bind RBCs at cool temperatures → agglutination → large rigid aggregates → peripheral vascular occlusion.
Cryoglobulinemia: similar temperature-dependent rigidity from immunoglobulin precipitation on RBC surface.
Hypothermia directly increases membrane rigidity and cytoplasmic viscosity → decreased deformability even without antibodies.
Board clue: Acrocyanosis worse in cold + hemolytic anemia + high-titer cold agglutinins → cold agglutinin disease.

Hemoglobin C Disease
HbC (β6 Glu→Lys) crystallizes within RBCs → increased cytoplasmic viscosity → rigid cells.
Characteristic finding: hemoglobin C crystals appear as dense rectangular bars within RBCs on blood smear.
Milder than sickle cell disease because HbC crystals form less readily than HbS polymers.
HbSC disease: coinheritance produces intermediate severity — both sickling and crystallization compromise deformability.

Artificial Surface Effects
Mechanical heart valves create high shear stress → RBC fragmentation → schistocytes with poor deformability.
Extracorporeal circulation (bypass, ECMO) → membrane damage from artificial surfaces → echinocyte formation → reduced deformability.
March hemoglobinuria: repetitive foot trauma → mechanical RBC destruction → fragments with compromised deformability.
Board pearl: New anemia after valve replacement + schistocytes on smear → mechanical hemolysis, not valve dysfunction.

Laboratory Assessment of Deformability
Osmotic fragility test: RBCs exposed to hypotonic saline. Spherocytes (poor deformability) lyse at higher osmolality than normal cells.
Ektacytometry: laser diffraction measures RBC deformation under shear stress — gold standard but not routinely available.
Blood smear morphology: spherocytes, elliptocytes, sickle cells, and fragments all indicate deformability defects.
Mean corpuscular hemoglobin concentration (MCHC): elevated in spherocytosis due to membrane loss.

Therapeutic Implications
Splenectomy: removes the filter that traps rigid cells. Effective for hereditary spherocytosis, less so for enzyme defects.
Hydroxyurea in sickle cell: increases HbF → reduces sickling → improves deformability → fewer vaso-occlusive crises.
Hydration therapy: reduces cytoplasmic viscosity in sickle cell crisis by decreasing MCHC.
Exchange transfusion: replaces rigid cells with normal deformable RBCs in severe sickle crisis or malaria.

Board Question Stem Patterns
Spherocytes + family history + negative Coombs test → hereditary spherocytosis.
Hemolysis after antimalarial in African American male → G6PD deficiency → oxidative rigidity.
Target cells + microcytosis + normal iron studies → thalassemia → altered SA:V ratio.
Sickle cells + pain crisis → HbS polymerization → vaso-occlusion from rigid cells.
Schistocytes + low platelets + renal failure → HUS → mechanical fragmentation.
Echinocytes + chronic hemolysis → pyruvate kinase deficiency → ATP depletion.
Acanthocytes + neurologic symptoms → abetalipoproteinemia → membrane lipid abnormality.

One-Line Recap
Erythrocyte deformability — determined by membrane elasticity (spectrin-actin network), surface area-to-volume ratio (biconcave shape), and cytoplasmic viscosity (hemoglobin concentration) — enables passage through narrow capillaries, with defects causing premature splenic destruction and hemolytic anemia in spherocytosis, sickle cell disease, enzyme deficiencies, and membrane disorders.

bottom of page