
eduo
visual
Endocrine
Cushing syndrome: diagnosis and management
Cushing syndrome = clinical manifestations of chronic glucocorticoid excess, regardless of source.
— Multiple features of hypercortisolism cluster together (especially catabolic signs: thin skin, wide purple striae, proximal myopathy, easy bruising)
— Unexplained osteoporosis in a young patient
— Adrenal incidentaloma with metabolic features
— Hypokalemic metabolic alkalosis in the right clinical context
— Exogenous glucocorticoids (most common overall — always exclude first)
— ACTH-dependent (~80% of endogenous): Cushing disease (pituitary adenoma ~70%), ectopic ACTH (small cell lung CA, carcinoid ~10%)
— ACTH-independent (~20%): adrenal adenoma, adrenal carcinoma, bilateral adrenal hyperplasia
Board pearl: The most common cause of Cushing syndrome is iatrogenic (exogenous steroids). The most common cause of endogenous Cushing syndrome is a pituitary corticotroph adenoma (Cushing disease).

History clues:
— Exogenous steroid use (oral, inhaled high-dose, topical potent, intra-articular)
— Rapid weight gain over months
— Family history of MEN-1 (pituitary tumors)
— Smoking history (ectopic ACTH — small cell lung cancer, bronchial carcinoid)
Key distinction: Discriminatory features (favor Cushing over simple obesity): purple striae >1 cm, proximal myopathy, easy bruising, unexplained osteoporosis.

— Wide (>1 cm) purple/violaceous striae — highly specific
— Thin, atrophic skin ("cigarette paper" quality)
— Ecchymoses without significant trauma
— Facial plethora
— Acanthosis nigricans (insulin resistance)
Board pearl: Hyperpigmentation + hypokalemia + very high cortisol → think ectopic ACTH secretion (often small cell lung cancer or bronchial carcinoid). These patients may present acutely without classic cushingoid habitus because the disease progresses rapidly.

Before any testing → rule out exogenous glucocorticoid use (history!).
First-line screening tests (need ≥2 abnormal for diagnosis):
Interpretation logic:
— Normal HPA axis: exogenous dex → ↓ ACTH → ↓ cortisol
— Cushing syndrome: cortisol remains elevated despite dex
Next best step: If clinical suspicion is high and initial screening is positive → confirm with a second test before proceeding to localization.
Board pearl: False positives on DST occur with: OCPs (↑ CBG), alcoholism (pseudo-Cushing), depression, obesity, sleep apnea, and CYP3A4 inducers (phenytoin, rifampin → rapid dex metabolism).

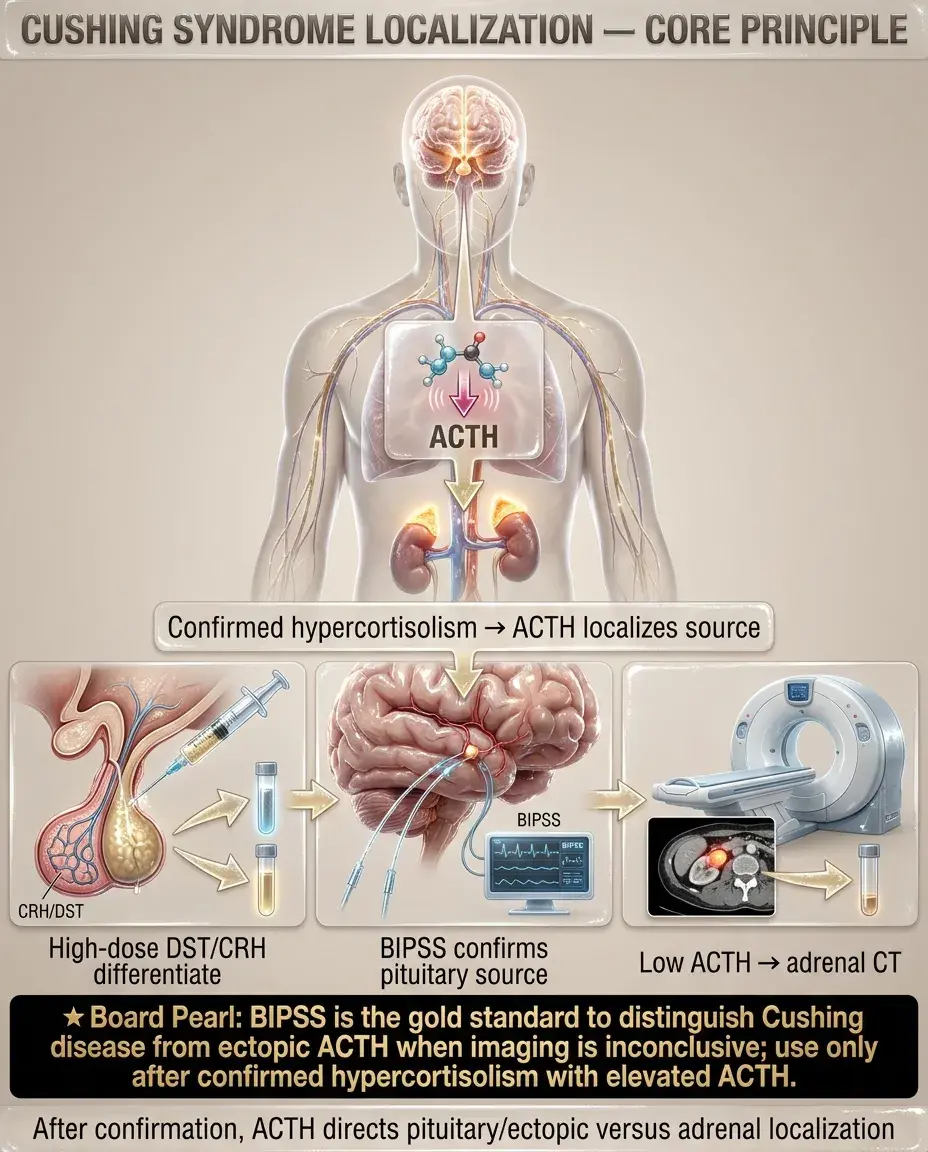
Once hypercortisolism is confirmed → measure plasma ACTH:
— Pituitary (Cushing disease) vs. ectopic ACTH
— Next best step: High-dose DST (8 mg overnight) or CRH stimulation test
◦ Cushing disease: cortisol suppresses >50% (pituitary adenoma retains partial feedback)
◦ Ectopic ACTH: no suppression (autonomous, no feedback sensitivity)
— Pituitary MRI with gadolinium: identifies adenoma (~60% sensitivity for microadenoma)
— If MRI negative or equivocal → bilateral inferior petrosal sinus sampling (BIPSS): gold standard to distinguish pituitary vs. ectopic
◦ Central-to-peripheral ACTH ratio ≥2:1 (basal) or ≥3:1 (after CRH) → pituitary source
— Adrenal source → CT abdomen
— Unilateral mass: adenoma (small, smooth) vs. carcinoma (large >4 cm, irregular, calcified)
— Bilateral enlargement: bilateral macronodular hyperplasia, PPNAD (primary pigmented nodular adrenal disease)
Board pearl: BIPSS is the gold standard for distinguishing Cushing disease from ectopic ACTH when imaging is inconclusive. It is NOT a screening test — only performed after hypercortisolism is confirmed and ACTH is elevated.
— Remission rates: 70–90% for microadenomas, lower for macroadenomas
— Postoperative assessment: serum cortisol <2 μg/dL within 72 hours indicates remission (adrenal suppression = the remaining normal corticotrophs were suppressed by chronic hypercortisolism)
— Patients need glucocorticoid replacement (hydrocortisone) postoperatively until HPA axis recovers (months to >1 year)
— Repeat TSS
— Radiation therapy (stereotactic radiosurgery or conventional): effect delayed 3–5 years; medical therapy needed as bridge
— Medical therapy (steroidogenesis inhibitors): ketoconazole, metyrapone, osilodrostat
— Bilateral adrenalectomy: definitive cure but last resort → lifelong adrenal insufficiency replacement + risk of Nelson syndrome (↑ ACTH → pituitary tumor enlargement + hyperpigmentation)
Next best step after confirmed Cushing disease: Refer to experienced pituitary neurosurgeon for TSS.

Ectopic ACTH syndrome:
— Medical adrenal blockade: ketoconazole, metyrapone, mitotane, etomidate (IV, for emergent control)
— Bilateral adrenalectomy if medical therapy fails and tumor is unresectable
Adrenal adenoma:
Adrenal carcinoma:
Bilateral adrenal hyperplasia (ACTH-independent macronodular hyperplasia, PPNAD):
Board pearl: Etomidate is the only IV agent that rapidly lowers cortisol — used in ICU settings for severe Cushing with life-threatening complications (sepsis, psychosis, uncontrolled hyperglycemia).

— Monitor LFTs (hepatotoxicity risk); drug interactions (CYP3A4 inhibitor)
— Side effects: ↑ androgens (hirsutism, acne), hypokalemia
— Slow onset; monitor drug levels; causes adrenal insufficiency
— Cannot monitor cortisol levels (receptor blocked, cortisol rises); monitor clinical improvement and glucose
— Major side effect: hyperglycemia (↓ insulin secretion)
Key distinction: Mifepristone blocks the cortisol receptor — serum cortisol and ACTH will ↑; titrate based on clinical response (glucose, weight, BP), NOT cortisol levels.

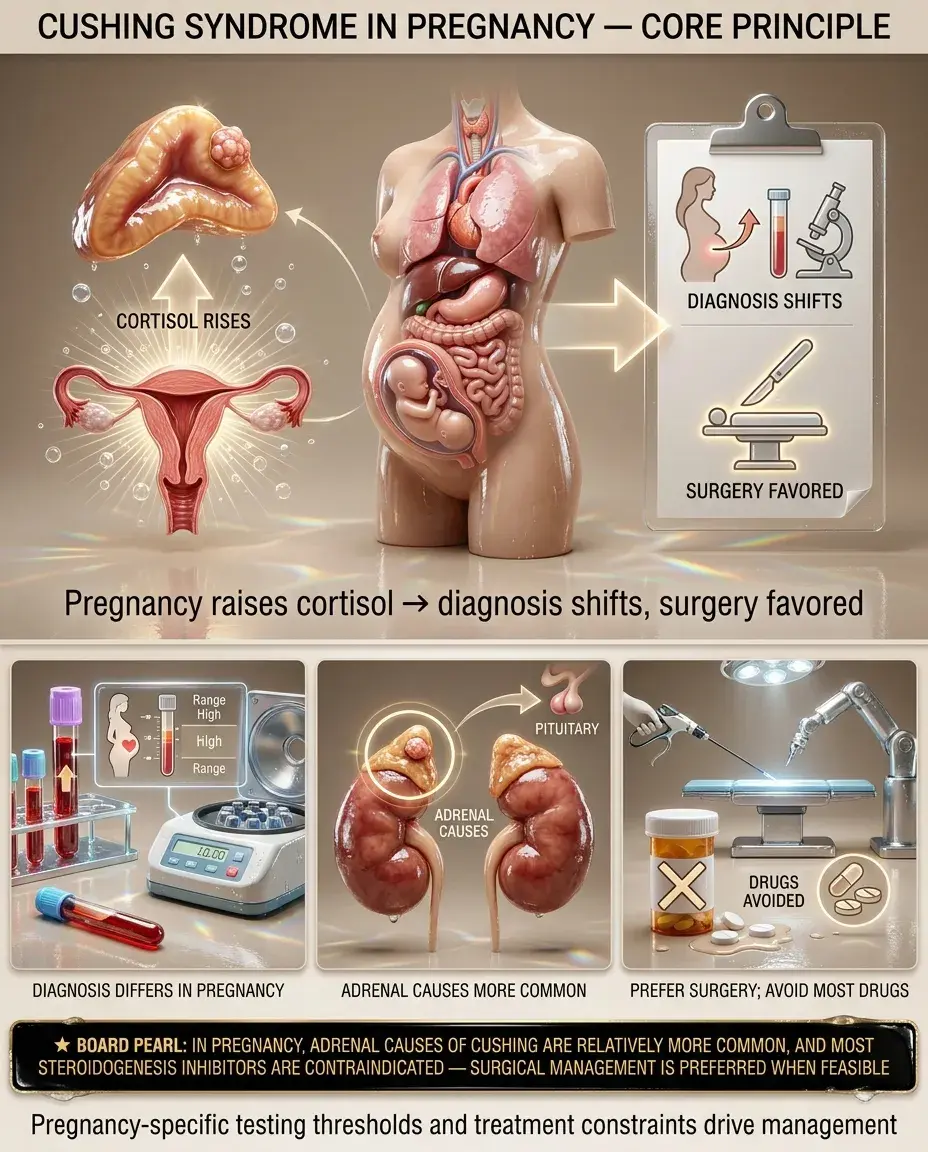
— Pregnancy normally ↑ cortisol (↑ CBG, placental CRH) → 24-hour UFC can be 2–3× upper normal in pregnancy
— UFC >3× ULN is suggestive in pregnancy
— Late-night salivary cortisol retains some utility
— DST is less reliable (altered dex metabolism in pregnancy)
Management:
Board pearl: In pregnancy, adrenal causes of Cushing are relatively more common, and most steroidogenesis inhibitors are contraindicated — surgical management is preferred when feasible.
Pediatric Cushing syndrome:
Elderly:
— CRH stimulation after low-dose DST (Dex-CRH test) helps differentiate
Board pearl: In a child with obesity + short stature (or growth arrest), suspect Cushing syndrome. Simple obesity in children is associated with normal or accelerated linear growth.

— Perioperative VTE prophylaxis is essential for Cushing patients undergoing surgery
— Consider PCP prophylaxis (TMP-SMX) when cortisol is very high
— Particularly severe in ectopic ACTH (very high cortisol levels)
Board pearl: Severe Cushing syndrome with K⁺ <3.0, alkalosis, and very high cortisol → think ectopic ACTH source until proven otherwise.

After successful treatment of Cushing syndrome (TSS, adrenalectomy), the HPA axis is suppressed:
Adrenal crisis:
Board pearl: Post-curative surgery for Cushing, feeling worse (fatigue, myalgia, arthralgias) is expected — "glucocorticoid withdrawal syndrome" — may persist for months; gradual taper and patient education are essential.

Pseudo-Cushing states mimic biochemical hypercortisolism without true autonomous cortisol excess:
How to distinguish:
Key distinction: In pseudo-Cushing, the HPA axis is functionally overactive but not autonomous. In true Cushing, there is autonomous cortisol production that escapes normal feedback.

— ↑ cortisol effects but ↓ ACTH, ↓ endogenous cortisol; synthetic steroids (prednisone, dexamethasone) may not be detected by cortisol assays → low measured cortisol with clinical Cushing features
— Always take a thorough medication history including topical, inhaled, intra-articular steroids
— Shares hirsutism, acne, menstrual irregularity, obesity
— Lacks catabolic features (striae, myopathy, bruising)
— Normal cortisol, ↑ androgens, ↑ LH:FSH ratio
— Central obesity, HTN, DM, dyslipidemia overlap
— Normal 24-hour UFC, normal late-night salivary cortisol, normal DST
— Mild autonomous cortisol secretion without overt Cushing phenotype
— Diagnosed by 1-mg DST (cortisol >1.8 μg/dL) + ↓ ACTH
— May contribute to HTN, DM, osteoporosis
— Consider surgery if metabolic comorbidities are attributable
Board pearl: Subclinical Cushing from an adrenal incidentaloma is increasingly tested — screen all adrenal incidentalomas with a 1-mg overnight DST.

Who should be screened for Cushing syndrome:
Screening approach:
Post-treatment surveillance:
Board pearl: Cushing disease can recur years after seemingly successful surgery — long-term biochemical surveillance is mandatory.

— Postop hydrocortisone (10–12 mg/m²/day); taper by 20–25% every 1–3 months guided by symptoms and AM cortisol
— Cosyntropin stimulation test: cortisol >18 μg/dL at 30 or 60 min → HPA axis recovered → can discontinue replacement
— DM may improve or resolve → ↓ insulin/oral hypoglycemic doses gradually
— HTN: antihypertensives may need reduction
— Osteoporosis: repeat DEXA at 1–2 years; consider bisphosphonate if persistent osteoporosis
— Psychiatric symptoms: may take months to improve; screen for ongoing depression
Next best step after surgical cure: Educate patient on stress dosing, taper plan, and need for long-term recurrence surveillance.

— Physicians must counsel patients on risks of long-term glucocorticoid therapy before initiating
— Never abruptly discontinue chronic steroids → adrenal crisis risk
— Document steroid taper plan; ensure all providers are aware
Board pearl: All patients on chronic exogenous glucocorticoids or post-Cushing glucocorticoid replacement must receive sick-day rules and carry emergency injectable hydrocortisone.

Board pearl: A patient with bilateral adrenalectomy for Cushing who develops progressive hyperpigmentation and enlarging pituitary mass → Nelson syndrome.


