
eduo
visual
Renal & Urinary
Chronic kidney disease: staging and management
Chronic kidney disease (CKD) → sustained structural or functional kidney abnormality for ≥3 months, defined by GFR <60 mL/min/1.73 m² or markers of kidney damage (albuminuria, abnormal sediment, structural abnormalities) regardless of GFR.
— Persistently ↑ serum creatinine or ↓ eGFR on two measurements ≥3 months apart
— Persistent albuminuria (UACR ≥30 mg/g on two of three specimens)
— Abnormal renal imaging: small echogenic kidneys, polycystic kidneys, cortical thinning
— Unexplained anemia, hyperkalemia, metabolic acidosis, hyperphosphatemia
Board pearl: A single ↑ creatinine does NOT equal CKD — chronicity (≥3 months) must be established. Always distinguish CKD from AKI by reviewing prior labs, kidney size on ultrasound (small = chronic), and presence of anemia/bone disease.

Key history to elicit:
— Duration of DM and glycemic control (diabetic nephropathy = #1 cause of CKD in U.S.)
— HTN duration and control (#2 cause — hypertensive nephrosclerosis)
— Family history: ADPKD, Alport syndrome, FSGS
— NSAID/nephrotoxin exposure (chronic interstitial nephritis)
— Recurrent UTIs, nephrolithiasis, BPH → obstructive uropathy
— Autoimmune diseases: SLE, vasculitis
— Prior AKI episodes — each episode ↑ risk of subsequent CKD
Next best step: In any patient with newly discovered ↓ eGFR, obtain prior creatinine values and renal ultrasound to assess chronicity and etiology.

Renal ultrasound clues:
— Small (<9 cm), echogenic kidneys → chronic parenchymal disease
— Normal or enlarged kidneys in CKD → consider DM nephropathy, amyloidosis, HIV-associated nephropathy, ADPKD
Board pearl: Normal-sized or large kidneys in a CKD patient should prompt consideration of diabetic nephropathy, infiltrative disease, or polycystic kidney disease — not all CKD kidneys are small.

— Confirm with repeat eGFR ≥3 months later to establish chronicity
— Cystatin C–based eGFR useful when creatinine unreliable (extremes of muscle mass, amputation, cirrhosis)
— Spot urine albumin-to-creatinine ratio (UACR) — preferred screening test
— A1 (normal): <30 mg/g
— A2 (moderately increased, formerly "microalbuminuria"): 30–300 mg/g
— A3 (severely increased): >300 mg/g
— Confirm on ≥2 of 3 specimens over 3–6 months (transient causes: fever, exercise, UTI)
Key distinction: 24-hour urine protein collection is less practical but still used when spot UACR is discordant or when quantifying non-albumin proteinuria (e.g., light chains in myeloma).

GFR stages:
Additional labs for all CKD patients:
Next best step: At CKD stage 3 and beyond, routinely monitor Ca²⁺, PO₄³⁻, PTH, Hgb, K⁺, and HCO₃⁻ — complications of CKD begin accumulating at this stage.

— Reduces intraglomerular pressure → slows progression
— Expect up to 30% ↑ in Cr after initiation — acceptable; do NOT stop unless >30% rise or hyperkalemia
— Monitor K⁺ and Cr within 1–2 weeks of starting/dose change
— Do NOT combine ACEi + ARB (↑ hyperkalemia, AKI risk, no added benefit — ONTARGET trial)
— Now first-line add-on for CKD with albuminuria regardless of DM status (DAPA-CKD, EMPA-KIDNEY trials)
— Reduce progression to ESKD, cardiovascular events, and HF hospitalizations
— Mechanism: afferent arteriole vasoconstriction → ↓ intraglomerular pressure
— Expect initial ↓ eGFR ("dip") — acceptable; reflects hemodynamic effect
— Can initiate if eGFR ≥20 mL/min
Board pearl: The combination of ACEi/ARB + SGLT2i is the cornerstone of renoprotective therapy in proteinuric CKD.

— Indicated for T2DM-associated CKD with persistent albuminuria despite max ACEi/ARB + SGLT2i
— Reduces CKD progression and cardiovascular events (FIDELIO-DKN, FIGARO-DKD)
— Monitor K⁺ closely — risk of hyperkalemia
— HbA1c target ~7% (individualize based on hypoglycemia risk)
— Metformin: reduce dose at eGFR 30–45; discontinue at <30
— SGLT2i: dual benefit (glycemic + renoprotective)
— GLP-1 receptor agonists: cardiovascular and possible renal benefit
— Avoid glyburide in CKD (active metabolites → hypoglycemia)
— Sodium restriction: <2 g/day (reduces proteinuria and BP)
— Protein intake: 0.8 g/kg/day in non-dialysis CKD (avoid excessive restriction)
— Smoking cessation: accelerates CKD progression
— Regular exercise, weight management
Next best step: After starting ACEi/ARB + SGLT2i, add finerenone if diabetic CKD with persistent albuminuria.

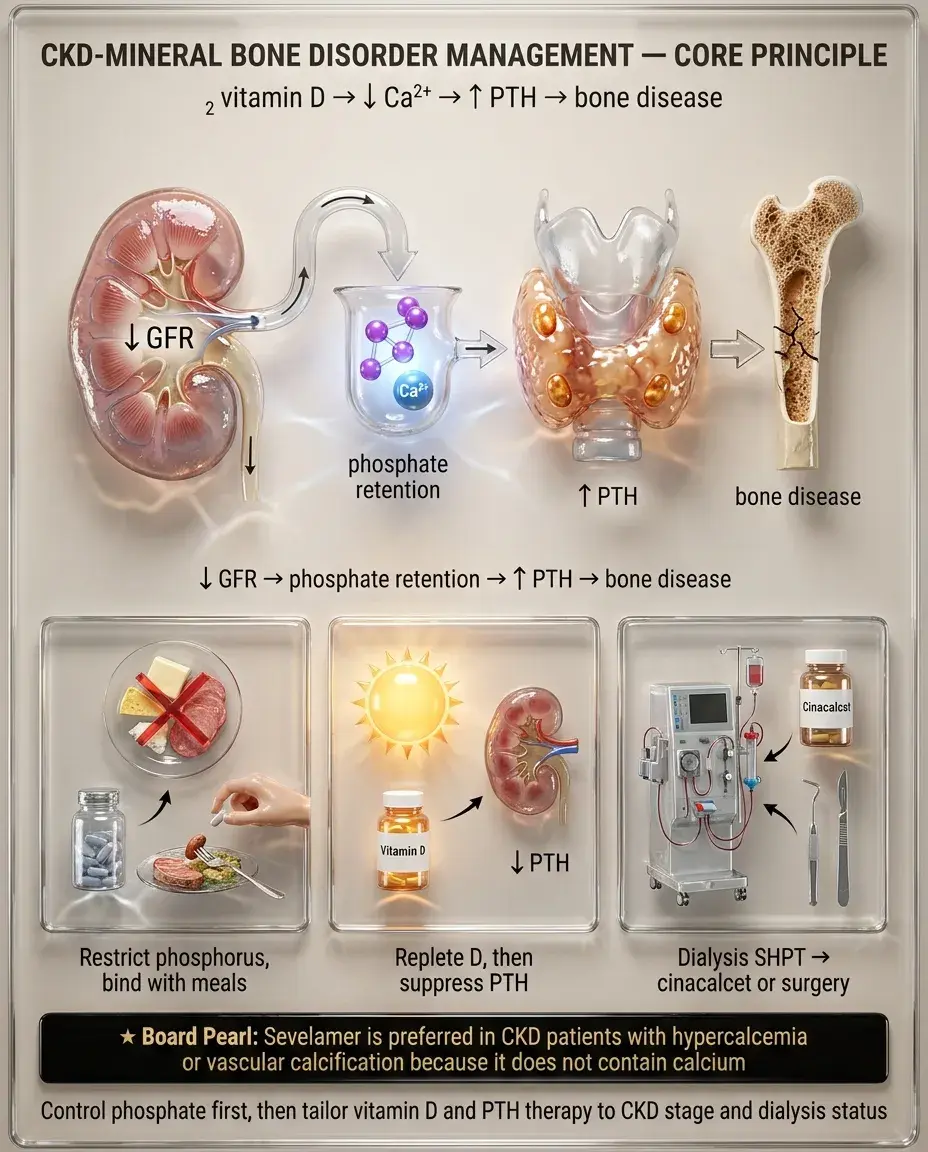
— Dietary phosphorus restriction (processed foods, dairy, cola)
— Phosphate binders with meals: calcium acetate, sevelamer (non-Ca²⁺ based — preferred if Ca²⁺ already ↑), lanthanum
— Target: normal serum phosphorus
— Replete 25-OH vitamin D deficiency with cholecalciferol/ergocalciferol
— Active vitamin D (calcitriol) or analogs (paricalcitol) for ↑ PTH in stages 4–5 when 25-OH D is replete
— In CKD G3–G5 (non-dialysis): trend PTH, treat if progressively rising
— On dialysis: target PTH roughly 2–9× upper limit of normal
— Cinacalcet (calcimimetic) for persistent secondary hyperparathyroidism on dialysis
— Parathyroidectomy for refractory tertiary hyperparathyroidism (autonomous PTH secretion with hypercalcemia)
Board pearl: Sevelamer is preferred in CKD patients with hypercalcemia or vascular calcification because it does not contain calcium.
Diabetic nephropathy:
Elderly patients:
Board pearl: Absence of diabetic retinopathy in a T2DM patient with nephrotic-range proteinuria should raise suspicion for a non-diabetic glomerular disease → renal biopsy indicated.

Pregnancy in CKD:
Pediatric CKD:
Board pearl: ACEi/ARB must be stopped immediately in any CKD patient who becomes pregnant — teratogenic effects occur in all trimesters.

Anemia of CKD:
— IV iron preferred in dialysis patients; oral or IV in non-dialysis CKD
— Start only after iron repletion if Hgb <10 g/dL
— Target Hgb 10–11.5 g/dL — do NOT target >13 (↑ cardiovascular events, stroke — CHOIR/TREAT trials)
— HIF-prolyl hydroxylase inhibitors (roxadustat): oral alternative
Metabolic acidosis:
Hyperkalemia:
Board pearl: Always correct iron deficiency before starting ESAs — iron-deficient erythropoiesis renders ESAs ineffective.

Nephrology referral:
Dialysis preparation:
Emergent dialysis indications (mnemonic-free approach):
Board pearl: Uremic pericarditis is an absolute indication for urgent dialysis regardless of other parameters.

Distinguishing CKD from AKI:
AKI superimposed on CKD:
Other causes of ↑ Cr without true GFR decline:
Key distinction: A patient with CKD whose Cr rises acutely after NSAID or contrast exposure has AKI on CKD — the acute component may be reversible.

Glomerular:
Tubulointerstitial:
Vascular:
Board pearl: Sudden ↑ Cr after starting ACEi in bilateral renal artery stenosis (or unilateral in a solitary kidney) → bilateral renovascular disease. Hold ACEi/ARB and obtain imaging (duplex US, MRA, or CTA).

— Serum creatinine → eGFR
— Spot UACR
— Statin therapy: moderate-to-high intensity for CKD stages 1–4 (atorvastatin preferred — not renally cleared)
— Statin benefit less clear in dialysis patients (4D, AURORA trials neutral) — continue if already on statin but no need to initiate
— Aspirin: individualized based on ASCVD risk
— Influenza (annually), pneumococcal (PCV20 or PCV15 + PPSV23), hepatitis B (high-dose formulation)
— COVID-19 vaccination + additional doses (immunocompromised protocol)
— CKD patients have impaired vaccine responses → check hepatitis B titers, revaccinate if non-responder
Board pearl: Gadolinium-based contrast is contraindicated in eGFR <30 due to risk of nephrogenic systemic fibrosis — use group II agents if absolutely necessary.

— G1–G2, A1: annual eGFR, UACR, BP
— G3a, A1–A2: every 6–12 months
— G3b–G4: every 3–6 months
— G5/dialysis: monthly or more frequent
— eGFR, UACR, BMP (K⁺, HCO₃⁻, Cr)
— BP assessment and medication reconciliation
— Assess medication dosing for renal clearance
— CBC for anemia
— Ca²⁺, PO₄³⁻, intact PTH (frequency ↑ with advancing stage)
— 25-OH vitamin D annually
— Lipids, HbA1c (if DM)
Next best step: If eGFR declining faster than expected, reassess medication adherence, check for ongoing nephrotoxin exposure, evaluate for superimposed AKI, obstruction, or new glomerular disease.

— Conservative management (no dialysis) is a valid option, especially in frail elderly with poor functional status and multiple comorbidities
— Discuss prognosis honestly — address goals of care early (ideally at CKD stage 4)
— Palliative care referral for symptom management in those choosing conservative care
— Document wishes regarding dialysis withdrawal, resuscitation status
— Dialysis withdrawal is the second most common cause of death in ESKD patients — counsel families
— Many drugs require dose adjustment or avoidance in CKD (DOACs, metformin, gabapentin, opioids)
— Pharmacy reconciliation at every visit
— NSAIDs: avoid in CKD stages 3–5 (accelerate progression, cause AKI, hyperkalemia)
— CKD disproportionately affects Black, Hispanic, and Native American populations
— eGFR equations have removed race coefficients (CKD-EPI 2021) to reduce disparities in diagnosis and referral
— Ensure equitable access to transplant evaluation
Board pearl: The 2021 CKD-EPI equation no longer includes a race coefficient — this change was made to ensure equitable diagnosis and referral for all patients.

Board pearl: Episodic gross hematuria during URIs with underlying CKD → think IgA nephropathy; post-infectious GN occurs 2–3 weeks AFTER infection.


