
eduo
visual
Emergency and Critical Care
Acute cyanosis in infants: evaluation and emergency management
Acute cyanosis in an infant — visible blue-purple discoloration of skin and mucous membranes — signals deoxygenated hemoglobin ≥ 3–5 g/dL in capillary blood and demands immediate evaluation.
→ Appearance: alert vs limp/unresponsive
→ Work of Breathing: retractions, grunting, nasal flaring, apnea
→ Circulation to Skin: central cyanosis vs peripheral acrocyanosis

→ Birth/first days of life → duct-dependent congenital heart lesion, persistent pulmonary hypertension of the newborn (PPHN), sepsis
→ Sudden onset in a previously well infant → foreign body aspiration, apparent life-threatening event (BRUE/ALTE), arrhythmia
→ Episodic with feeding → tetralogy of Fallot (tet spell), vascular ring

→ Pre-ductal SpO₂ > post-ductal SpO₂ by ≥3% → right-to-left ductal shunt (PPHN, coarctation variants)
→ BP gradient: upper > lower extremity by >20 mmHg → coarctation of the aorta

The hyperoxia test is the cornerstone bedside tool to differentiate cardiac from pulmonary causes of cyanosis.
→ PaO₂ > 200 mmHg → pulmonary cause likely (V/Q mismatch responds to O₂)
→ PaO₂ 100–200 mmHg → indeterminate; consider PPHN, large intracardiac shunt
→ PaO₂ < 100 mmHg (and especially < 50 mmHg) → strongly suggests fixed right-to-left shunt (cyanotic CHD)

→ "Egg on a string" → TGA (narrow mediastinum, egg-shaped heart)
→ "Boot-shaped heart" → tetralogy of Fallot
→ ↑ pulmonary blood flow (cardiomegaly, pulmonary edema) → total anomalous pulmonary venous return (TAPVR), truncus arteriosus
→ ↓ pulmonary blood flow → tetralogy, pulmonary atresia, tricuspid atresia
→ Diffuse bilateral opacities → pneumonia, RDS, pulmonary hemorrhage

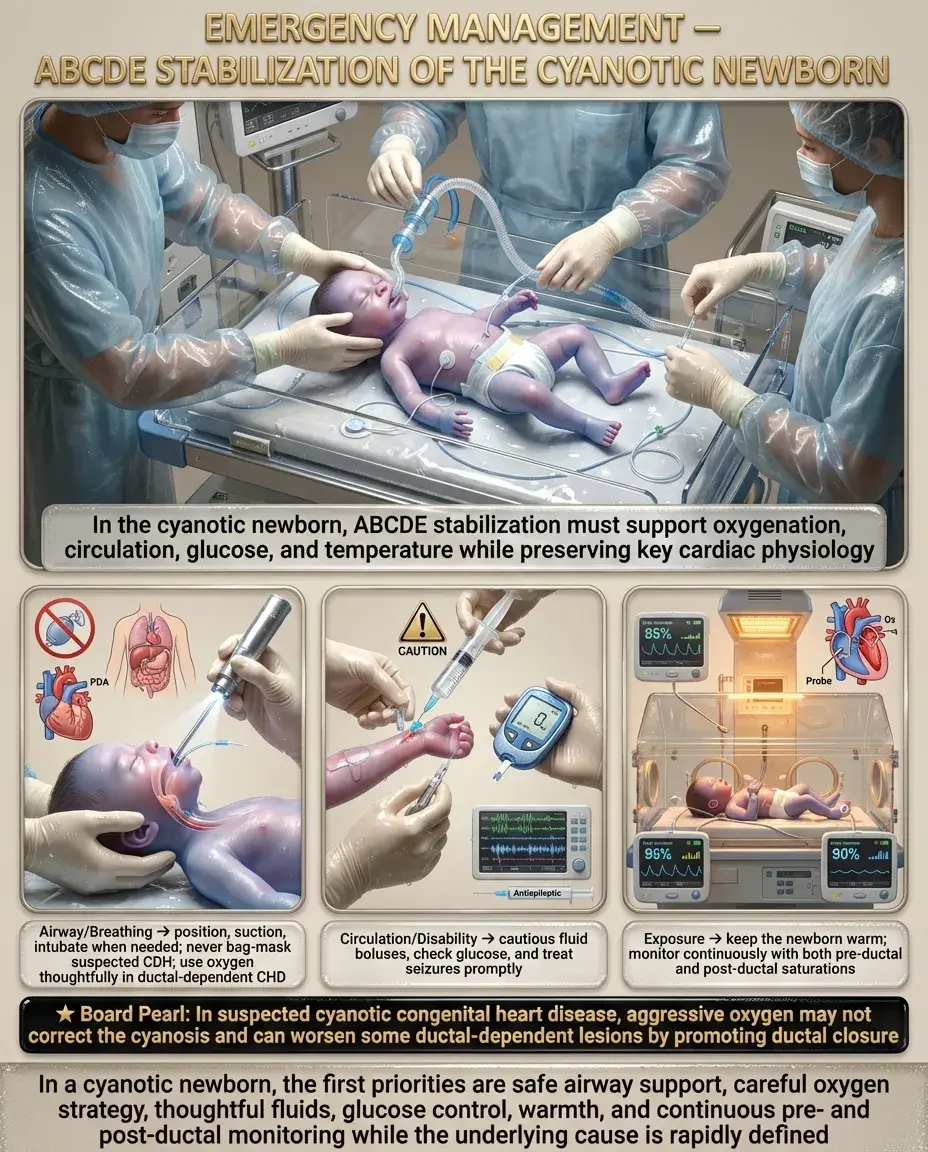
Immediate stabilization follows ABCDE approach:
→ In suspected CDH: intubate immediately, do NOT bag-mask (inflates stomach/bowel)
→ Clinical tip: In suspected cyanotic CHD, avoid aggressive O₂ — it will NOT fix the cyanosis and may worsen hemodynamics in some ductal-dependent lesions by closing the PDA
PGE₁ (alprostadil) is the critical intervention for duct-dependent cyanotic heart lesions.


→ Fail: SpO₂ < 90% in either extremity on any screen → immediate evaluation
→ Fail: SpO₂ 90–94% or >3% difference between pre- and post-ductal on 3 screens separated by 1 hour → echocardiography

→ Progressive dynamic RVOT obstruction worsens as infant grows

→ Hypoxic-ischemic encephalopathy from prolonged hypoxemia
→ Metabolic (lactic) acidosis → ↓ cardiac contractility → cardiovascular collapse
→ End-organ injury: renal failure, hepatic necrosis, NEC
→ Worsening metabolic acidosis (pH < 7.2, lactate ↑↑)
→ Bradycardia (terminal sign in infants)
→ Hypotension, mottled/gray appearance
→ Altered consciousness → limpness

→ Any infant with central cyanosis unresponsive to supplemental O₂
→ Suspected duct-dependent CHD requiring PGE₁ infusion
→ PPHN requiring iNO or high-frequency ventilation
→ Septic shock requiring vasopressors
→ Start PGE₁ BEFORE transfer — do not wait for echocardiographic confirmation if clinical suspicion is high
→ Ensure airway management capability during transport (PGE₁ → apnea risk)

Systematic approach to differential diagnosis of acute cyanosis:
→ Cyanotic CHD (5 T's): Tetralogy of Fallot, Transposition of Great Arteries, Tricuspid Atresia, Truncus Arteriosus, Total Anomalous Pulmonary Venous Return
→ PPHN (functional R→L shunting through PDA/PFO)
→ Myocarditis, cardiomyopathy → cardiogenic shock with poor perfusion
→ Pneumonia, RDS, bronchiolitis, foreign body aspiration, pneumothorax, pleural effusion, CDH
→ Methemoglobinemia (acquired > congenital), carbon monoxide poisoning (SpO₂ falsely normal)
→ Central apnea (prematurity, seizures, intracranial hemorrhage, brainstem lesion)
→ TGA: severe cyanosis from BIRTH, "egg on string" CXR, ↑ pulmonary blood flow; needs PGE₁ ± septostomy
→ TOF: may be pink at birth, progressive cyanosis over weeks-months; episodic tet spells; "boot-shaped" heart on CXR; ↓ pulmonary blood flow
→ Both fail hyperoxia test
→ PPHN: pre-/post-ductal SpO₂ gradient >3%, history of perinatal stress (meconium, asphyxia, CDH), echo shows structurally normal heart with R→L shunting
→ CHD: structural abnormality on echo
→ Overlap is significant in neonates; both may present with cyanosis, poor feeding, lethargy
→ Clinical tip: Treat BOTH simultaneously until differentiated — start antibiotics AND PGE₁ in a critically ill cyanotic neonate
→ SpO₂ ~85% that does not change with O₂; chocolate-brown blood that does not turn red when exposed to O₂; confirm with co-oximetry

→ Universal newborn pulse oximetry screen is performed at ≥24 hours of life in the well-baby nursery
→ Targets 7 lesions: HLHS, pulmonary atresia, tetralogy of Fallot, TAPVR, TGA, tricuspid atresia, truncus arteriosus
→ Also detects: critical coarctation, others with ↓ SpO₂

→ Infants with cyanotic CHD are at ↑ risk for neurodevelopmental delay → early intervention referral

→ Provide clear, jargon-free explanations with diagrams of the heart defect
→ Connect families with support organizations (e.g., Mended Little Hearts)
→ Trisomy 21 → AV canal, VSD, TOF
→ 22q11 deletion (DiGeorge) → truncus arteriosus, interrupted aortic arch, TOF
→ Turner syndrome (45,X) → coarctation, bicuspid aortic valve



