top of page

eduo
visual

Behavioral Health & Nervous System
Visual Pathways and Field Defects
Core Principle of Visual Pathways
🧷
Light information travels from retina → optic nerve → optic chiasm → optic tract → lateral geniculate nucleus (LGN) → optic radiations → primary visual cortex (V1).
🧷
Each eye's visual field divides into nasal (medial) and temporal (lateral) hemifields, with nasal fibers crossing at the chiasm while temporal fibers remain ipsilateral.
🧷
This crossing pattern means the right brain processes the left visual field from both eyes, and the left brain processes the right visual field from both eyes.
🧷
Understanding fiber anatomy at each level predicts the specific visual field defect pattern when lesions occur at different points along the pathway.

Retinal Organization and Visual Field Mapping
📍
The retina inverts the visual world: superior visual field → inferior retina, inferior visual field → superior retina, temporal field → nasal retina, nasal field → temporal retina.
📍
The fovea represents central vision with highest acuity, while the peripheral retina detects motion and dim light.
📍
Visual field testing maps what each eye sees independently, with the blind spot corresponding to the optic disc where ganglion cell axons exit.
📍
Board pearl: Visual field defects are described based on what the patient cannot see, not the anatomical location of retinal damage.

Optic Nerve Lesions
🔹
Unilateral optic nerve damage → ipsilateral monocular vision loss affecting all visual fields in that eye.
🔹
Common causes: optic neuritis (demyelination), ischemic optic neuropathy, compression by tumor, trauma, or glaucoma.
🔹
The pupillary light reflex shows an afferent pupillary defect (Marcus Gunn pupil) — the affected pupil paradoxically dilates when light swings from normal to affected eye.
🔹
Central scotoma (blind spot in central vision) suggests optic neuritis, while altitudinal defects (loss of superior or inferior half) suggest vascular etiology.
🔹
Board clue: Young woman with painful monocular vision loss that improves over weeks → optic neuritis, consider multiple sclerosis.

Optic Chiasm and Bitemporal Hemianopia
⭐
At the chiasm, nasal retinal fibers (temporal visual fields) from both eyes cross while temporal retinal fibers (nasal visual fields) remain ipsilateral.
⭐
Chiasmal compression → bitemporal hemianopia (loss of both temporal visual fields), creating "tunnel vision."
⭐
Classic cause: pituitary adenoma compressing chiasm from below. Other causes include craniopharyngioma, meningioma, aneurysm.
⭐
Board pearl: Bitemporal hemianopia is pathognomonic for chiasmal lesion — no other lesion produces this pattern.
⭐
Associated findings depend on cause: amenorrhea/galactorrhea (prolactinoma), acromegaly (GH adenoma), Cushing's features (ACTH adenoma).

Optic Tract and Homonymous Hemianopia
✅
Beyond the chiasm, each optic tract carries fibers from the ipsilateral temporal retina and contralateral nasal retina → information from the contralateral visual field.
✅
Optic tract lesion → contralateral homonymous hemianopia (same-sided visual field loss in both eyes).
✅
The defect is "incongruous" — the field losses don't perfectly match between eyes because nasal and temporal fibers haven't fully mixed.
✅
Rare compared to other locations; usually from stroke, tumor, or trauma affecting the cerebral peduncle region.
✅
Board distinction: Optic tract lesions also cause contralateral afferent pupillary defect due to asymmetric pupillary fiber damage.

Lateral Geniculate Nucleus Anatomy
🧠
The LGN in the thalamus has six layers: layers 1-2 receive magnocellular input (motion/contrast), layers 3-6 receive parvocellular input (color/detail).
🧠
Retinotopic organization is maintained — superior retina → medial LGN, inferior retina → lateral LGN.
🧠
Blood supply comes from the anterior choroidal artery (lateral portion) and posterior cerebral artery (medial portion).
🧠
LGN lesions produce contralateral homonymous hemianopia that is more congruous than optic tract lesions.
🧠
Isolated LGN lesions are rare; usually occur with thalamic strokes affecting adjacent structures.

Optic Radiations: Meyer's Loop and Baum's Loop
⚡
Optic radiations split into two pathways from LGN to occipital cortex.
⚡
Meyer's loop: inferior fibers (superior visual field) travel anteriorly through temporal lobe before reaching inferior occipital cortex.
⚡
Baum's loop: superior fibers (inferior visual field) travel directly through parietal lobe to superior occipital cortex.
⚡
This anatomical separation explains why temporal lobe lesions cause "pie in the sky" defects while parietal lesions cause "pie on the floor" defects.
⚡
Board pearl: Anterior temporal lobectomy for epilepsy risks Meyer's loop damage → contralateral superior quadrantanopia.

Primary Visual Cortex (V1) Organization
📌
V1 (Brodmann area 17) in the occipital lobe maintains precise retinotopic mapping along the calcarine sulcus.
📌
Superior bank of calcarine → inferior visual field; inferior bank → superior visual field.
📌
The occipital pole represents central/macular vision, while anterior calcarine represents peripheral vision.
📌
Blood supply: posterior cerebral artery (PCA), with the occipital pole having dual supply from PCA and middle cerebral artery.
📌
This dual supply explains macular sparing in PCA strokes — central vision preserved despite peripheral field loss.

Cortical Visual Field Defects
📣
Occipital cortex lesions produce contralateral homonymous hemianopia with perfect congruity between eyes.
📣
Bilateral occipital lesions → cortical blindness with preserved pupillary reflexes (afferent pathway through pretectal area intact).
📣
Anton syndrome: bilateral occipital damage with denial of blindness — patients confabulate visual experiences.
📣
Riddoch phenomenon: motion perception preserved despite loss of form vision in the blind field.
📣
Board pearl: Homonymous hemianopia with normal pupillary reflexes localizes the lesion posterior to the LGN.

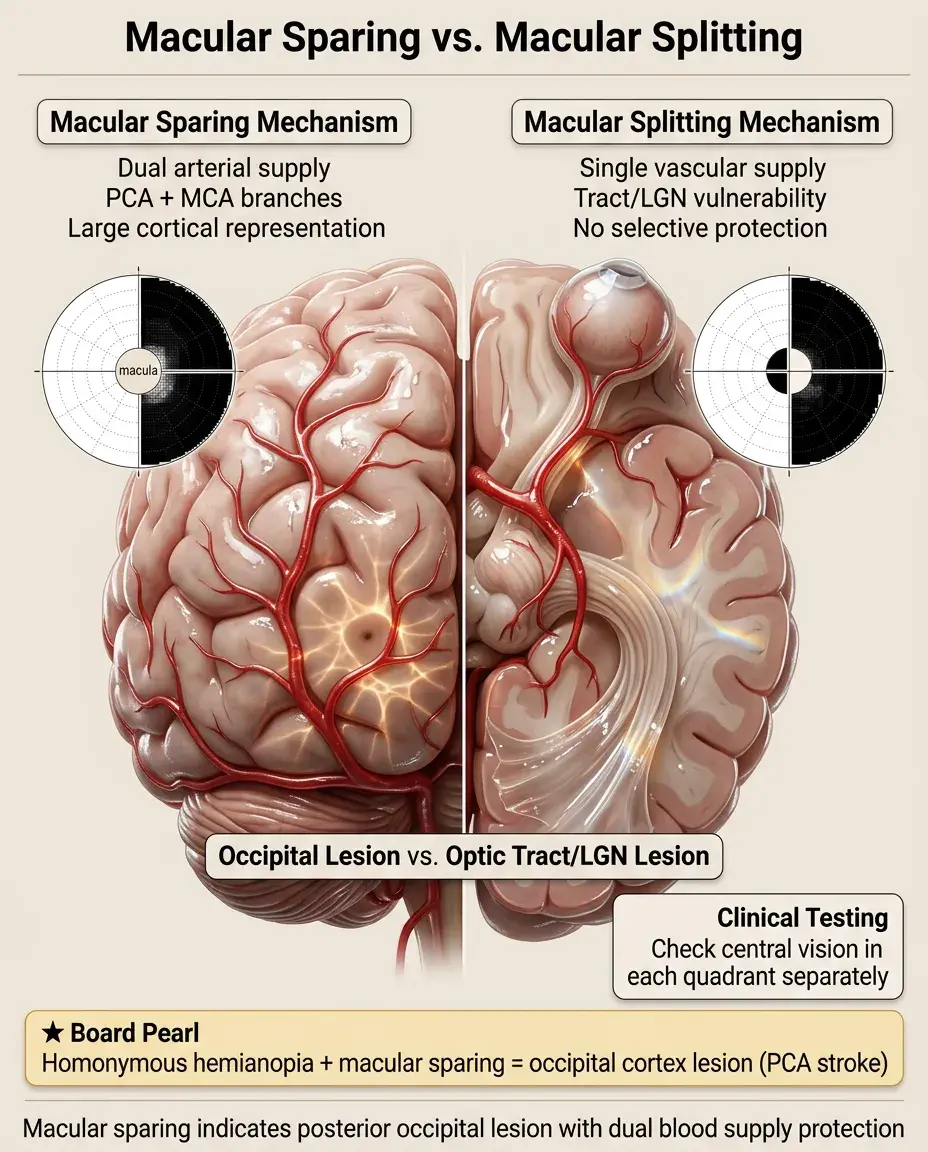
Macular Sparing vs. Macular Splitting
🔸
Macular sparing: central vision preserved in homonymous hemianopia, typically from posterior occipital lesions due to dual arterial supply.
🔸
Macular splitting: central vision affected equally with peripheral vision, seen in optic tract and LGN lesions.
🔸
The macula's large cortical representation and dual blood supply make it relatively resistant to complete infarction.
🔸
Testing tip: always check central vision separately in each quadrant to detect macular involvement.
🔸
Board clue: Homonymous hemianopia with macular sparing strongly suggests occipital cortex lesion from PCA stroke.
Quadrantanopias and Localizing Value
🧷
Superior quadrantanopia ("pie in the sky"): Meyer's loop lesion in temporal lobe — think temporal lobe epilepsy, tumor, or middle cerebral artery stroke.
🧷
Inferior quadrantanopia ("pie on the floor"): Baum's loop lesion in parietal lobe — often with contralateral sensory loss or neglect.
🧷
Checkerboard field defects: multiple small lesions or early compression — consider demyelination or infiltrative process.
🧷
Quadrantic defects are always homonymous (affecting same quadrant in both eyes) when from retrochiasmal lesions.
🧷
Board pearl: Isolated quadrantanopia without other neurological signs suggests optic radiation involvement.

Pupillary Light Reflex Pathway
📍
Light → retina → optic nerve → pretectal nucleus (not LGN) → bilateral Edinger-Westphal nuclei → oculomotor nerve → pupillary constriction.
📍
The pretectal bypass means cortical blindness preserves pupillary reflexes while optic nerve lesions eliminate them.
📍
Afferent pupillary defect indicates asymmetric optic nerve function — swinging flashlight test reveals paradoxical dilation.
📍
Light shown in one eye constricts both pupils equally (consensual response) due to bilateral pretectal connections.
📍
Board distinction: Pupillary reflexes intact + complete blindness = cortical; absent reflexes + blindness = anterior to LGN.

Visual Field Testing Methods
🔹
Confrontation testing: quick bedside screen where examiner compares patient's field to their own — misses subtle defects.
🔹
Goldmann perimetry: kinetic testing with moving targets of varying size/intensity — good for peripheral fields.
🔹
Humphrey automated perimetry: static testing with fixed points of varying brightness — gold standard for detecting early glaucoma.
🔹
Amsler grid: tests central 10 degrees for metamorphopsia (distortion) in macular disease.
🔹
Board pearl: Formal perimetry required to document field defects for disability or driving assessments.

Glaucomatous Visual Field Progression
⭐
Early: paracentral scotomas and nasal step (horizontal defect respecting horizontal meridian).
⭐
Moderate: arcuate scotomas following nerve fiber layer anatomy from blind spot to nasal horizontal meridian.
⭐
Advanced: superior and inferior arcuate defects merge → ring scotoma sparing central and temporal islands.
⭐
End-stage: only central island and temporal crescent remain before complete blindness.
⭐
Board clue: Visual field defects respecting horizontal meridian = glaucoma or other optic nerve pathology; respecting vertical meridian = neurological.

Vascular Patterns of Field Loss
✅
Anterior ischemic optic neuropathy (AION): sudden inferior or superior altitudinal defect from small vessel disease.
✅
Central retinal artery occlusion: complete monocular blindness except possibly cilioretinal artery supply to fovea.
✅
Branch retinal artery occlusion: sectoral field defect corresponding to affected vascular territory.
✅
Posterior cerebral artery stroke: contralateral homonymous hemianopia with macular sparing.
✅
Board pearl: Sudden painless monocular vision loss in elderly patient → consider vascular causes first.

Functional vs. Organic Visual Loss
🧠
Functional (non-organic): visual complaints without anatomical correlation — common in conversion disorder or malingering.
🧠
Testing reveals inconsistencies: different acuities at same distance, tubular fields that don't expand with distance, spiral or star-shaped fields.
🧠
Optokinetic nystagmus present despite claimed blindness proves intact visual pathway.
🧠
Stereoacuity requires binocular vision — if present, rules out monocular blindness.
🧠
Board approach: Normal pupillary reflexes + inconsistent examination = functional visual loss.

Pediatric Visual Pathway Disorders
⚡
Optic nerve hypoplasia: small optic disc, associated with septo-optic dysplasia (absent septum pellucidum, pituitary dysfunction).
⚡
Morning glory disc anomaly: enlarged, excavated disc with radial vessels — risk of retinal detachment.
⚡
Optic nerve glioma: slow-growing tumor in children with neurofibromatosis type 1 → proptosis and vision loss.
⚡
Cortical visual impairment: most common cause of bilateral vision loss in children — from hypoxic-ischemic injury.
⚡
Board pearl: Child with nystagmus and normal-appearing eyes → consider optic nerve hypoplasia or albinism.

Higher Cortical Visual Syndromes
📌
Prosopagnosia: inability to recognize faces despite normal vision — bilateral inferior occipitotemporal lesions.
📌
Achromatopsia: complete color blindness from bilateral V4 lesions — different from congenital color blindness.
📌
Akinetopsia: motion blindness from bilateral MT/V5 lesions — world appears as series of still frames.
📌
Balint syndrome: simultanagnosia (seeing parts but not wholes), optic ataxia, ocular apraxia — bilateral parieto-occipital lesions.
📌
Visual agnosia: cannot recognize objects despite normal acuity — ventral stream ("what" pathway) disruption.

Board Question Stem Patterns
📣
Bilateral temporal field loss in woman with amenorrhea → pituitary adenoma compressing chiasm.
📣
"Pie in the sky" defect after temporal lobectomy → Meyer's loop injury.
📣
Homonymous hemianopia with macular sparing and normal pupils → PCA stroke affecting occipital cortex.
📣
Monocular vision loss with afferent pupillary defect → optic nerve pathology.
📣
Child with poor vision but normal-appearing fundus → cortical visual impairment or optic nerve hypoplasia.
📣
Elderly patient with inferior altitudinal defect and disc swelling → anterior ischemic optic neuropathy.
📣
Visual field defect respecting vertical midline → retrochiasmal lesion; respecting horizontal midline → prechiasmal.

One-Line Recap
🔸
Visual pathway lesions produce predictable field defects: monocular loss (optic nerve), bitemporal hemianopia (chiasm), homonymous defects (retrochiasmal), with pupillary reflexes distinguishing anterior lesions from cortical blindness, and the vertical meridian rule separating neurological from ophthalmological causes.

bottom of page