top of page

eduo
visual

Multisystem Processes & Disorders
Tumor Markers
Core Principle of Tumor Markers
🧷
Tumor markers are substances produced by cancer cells or by normal cells in response to cancer that can be detected in blood, urine, or tissue.
🧷
They serve multiple clinical purposes: screening (rarely), diagnosis (in specific contexts), monitoring treatment response, detecting recurrence, and determining prognosis.
🧷
No single tumor marker is perfectly sensitive or specific — most can be elevated in benign conditions, inflammation, or normal physiological states.
🧷
The key to board questions is recognizing which markers are used for which cancers and understanding their limitations.
🧷
Board pearl: Tumor markers are primarily used for monitoring known cancer, not for screening asymptomatic populations.

AFP (Alpha-Fetoprotein): The Fetal Protein
📍
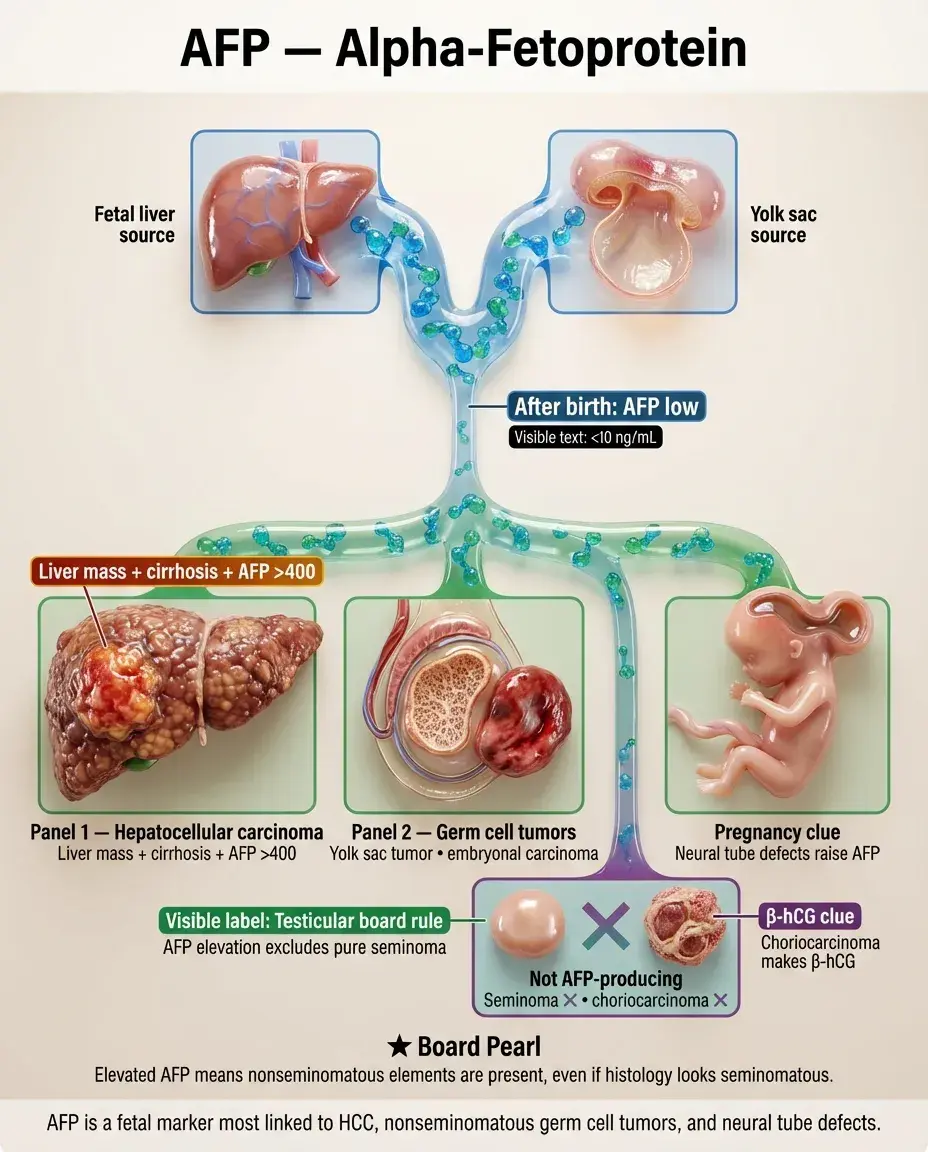
AFP is normally produced by fetal liver and yolk sac; levels drop to < 10 ng/mL after birth.
📍
Major associations: hepatocellular carcinoma (HCC), nonseminomatous germ cell tumors (yolk sac tumor, embryonal carcinoma), and neural tube defects in pregnancy.
📍
In HCC, AFP > 400 ng/mL is virtually diagnostic in the setting of a liver mass and cirrhosis.
📍
For testicular cancer, AFP elevation excludes pure seminoma — if AFP is elevated, the tumor contains nonseminomatous elements regardless of histology.
📍
Board distinction: Seminomas never produce AFP; choriocarcinomas never produce AFP (they make β-hCG).
CEA (Carcinoembryonic Antigen): The Colon Cancer Monitor
🔹
CEA is a glycoprotein involved in cell adhesion, normally produced during fetal development.
🔹
Primary use: monitoring colorectal cancer after resection — rising levels suggest recurrence before clinical or radiographic evidence appears.
🔹
Also elevated in other GI malignancies (pancreatic, gastric), lung cancer, breast cancer, and medullary thyroid cancer.
🔹
Non-malignant causes: smoking (most common), inflammatory bowel disease, pancreatitis, cirrhosis, COPD.
🔹
Board pearl: CEA is not used for screening colorectal cancer — it lacks sensitivity and specificity for early disease.

CA 19-9: The Pancreatic Marker
⭐
CA 19-9 is a sialylated Lewis A blood group antigen; individuals who are Lewis antigen-negative (7% of population) cannot produce it.
⭐
Primary association: pancreatic adenocarcinoma — levels correlate with tumor burden and prognosis.
⭐
Also elevated in other GI malignancies (cholangiocarcinoma, gastric, colorectal) and benign conditions (cholangitis, pancreatitis, cirrhosis).
⭐
Utility includes assessing resectability (very high levels suggest unresectable disease) and monitoring for recurrence after treatment.
⭐
Board clue: Patient with obstructive jaundice and CA 19-9 > 1000 U/mL → think pancreatic cancer.

CA-125: The Ovarian Cancer Marker
✅
CA-125 is a glycoprotein expressed by cells derived from coelomic epithelium (peritoneum, pleura, pericardium, ovarian epithelium).
✅
Primary use: monitoring epithelial ovarian cancer — levels correlate with disease burden and treatment response.
✅
Elevated in 80% of advanced ovarian cancer but only 50% of early-stage disease — not suitable for screening.
✅
Non-malignant causes: any process irritating the peritoneum — endometriosis, PID, pregnancy, menstruation, cirrhosis with ascites.
✅
Board pearl: In a postmenopausal woman with an adnexal mass and elevated CA-125, the next step is surgical evaluation, not observation.

PSA (Prostate-Specific Antigen): The Controversial Screening Tool
🧠
PSA is a serine protease produced by prostatic epithelium that liquefies semen; it is prostate-specific but not cancer-specific.
🧠
Elevated in prostate cancer, BPH, prostatitis, after ejaculation, and with prostate manipulation (DRE, biopsy, catheterization).
🧠
PSA exists in free and complexed forms; prostate cancer produces more complexed PSA → low free:total PSA ratio suggests malignancy.
🧠
Age-specific ranges and PSA velocity (rate of rise) help improve specificity.
🧠
Board controversy: Screening asymptomatic men remains debated due to overdiagnosis of indolent cancers and harm from unnecessary biopsies.

β-hCG (Beta-Human Chorionic Gonadotropin): Beyond Pregnancy
⚡
β-hCG is produced by syncytiotrophoblasts in pregnancy and by certain tumors.
⚡
Malignant associations: gestational trophoblastic disease (complete/partial mole, choriocarcinoma), germ cell tumors (choriocarcinoma, embryonal carcinoma), and rarely other cancers.
⚡
In testicular cancer, markedly elevated β-hCG (> 50,000 mIU/mL) suggests choriocarcinoma; mild elevations occur in embryonal carcinoma.
⚡
The β-subunit is measured because it's specific to hCG; the α-subunit is shared with LH, FSH, and TSH.
⚡
Board pearl: Young man with lung metastases and elevated β-hCG → think testicular choriocarcinoma, not lung cancer.

Calcitonin and Thyroid Cancer
📌
Calcitonin is produced by parafollicular C cells of the thyroid; it's the specific marker for medullary thyroid carcinoma (MTC).
📌
In MTC, calcitonin levels correlate with tumor burden and are used for screening in MEN2 families, confirming diagnosis, and monitoring after thyroidectomy.
📌
Pentagastrin or calcium stimulation testing can unmask early MTC when basal calcitonin is normal.
📌
CEA is often co-elevated in MTC and portends a worse prognosis.
📌
Board distinction: Papillary and follicular thyroid cancers produce thyroglobulin, not calcitonin; MTC produces calcitonin, not thyroglobulin.

LDH (Lactate Dehydrogenase): The Nonspecific Marker
📣
LDH catalyzes the interconversion of lactate and pyruvate; it's present in all tissues, making it highly nonspecific.
📣
Key cancer associations: testicular germ cell tumors (especially seminoma), lymphomas, leukemias, and melanoma.
📣
In testicular cancer, LDH is part of the S classification system along with AFP and β-hCG — elevated levels indicate higher stage.
📣
In lymphoma, LDH reflects tumor burden and cell turnover — it's a prognostic factor in many lymphoma scoring systems.
📣
Board pearl: LDH is too nonspecific to diagnose cancer but is useful for staging and prognosis in specific cancer types.

S-100 and Melanoma
🔸
S-100 is a calcium-binding protein expressed by cells of neural crest origin — melanocytes, Schwann cells, glial cells, chondrocytes.
🔸
Primary use: immunohistochemical marker for melanoma diagnosis and monitoring metastatic disease.
🔸
Also positive in nerve sheath tumors, gliomas, Langerhans cell histiocytosis, and certain sarcomas.
🔸
Serum S-100 levels correlate with melanoma tumor burden and can detect recurrence before clinical evidence.
🔸
Board clue: Immunohistochemistry positive for S-100 and HMB-45 → melanoma; S-100 positive but HMB-45 negative → consider other neural crest tumors.

Chromogranin A and Neuroendocrine Tumors
🧷
Chromogranin A is stored in secretory vesicles of neuroendocrine cells and released with hormones.
🧷
Major associations: carcinoid tumors, pheochromocytomas, pancreatic neuroendocrine tumors, small cell lung cancer, medullary thyroid carcinoma.
🧷
Levels correlate with tumor burden and can monitor treatment response in functional and nonfunctional neuroendocrine tumors.
🧷
False positives: proton pump inhibitor use (most common cause), renal insufficiency, heart failure, inflammatory conditions.
🧷
Board pearl: Stop PPIs for at least 2 weeks before measuring chromogranin A to avoid false elevation.

Immunoglobulins and Hematologic Malignancies
📍
Monoclonal immunoglobulin production is the hallmark of plasma cell disorders and some B-cell lymphomas.
📍
Multiple myeloma: monoclonal spike (M-spike) on serum protein electrophoresis, usually IgG or IgA; light chains detected in urine (Bence Jones proteins).
📍
Waldenström macroglobulinemia: IgM monoclonal gammopathy with hyperviscosity syndrome.
📍
Serum free light chain assay detects κ and λ light chains; an abnormal κ:λ ratio indicates monoclonal production.
📍
Board distinction: MGUS has M-spike < 3 g/dL and < 10% plasma cells; multiple myeloma has higher values plus end-organ damage (CRAB criteria).

CD Markers and Leukemia/Lymphoma
🔹
CD (cluster of differentiation) markers are cell surface proteins used to identify and classify hematologic malignancies by flow cytometry.
🔹
Key associations: CD20 (B cells) → B-cell lymphomas, target of rituximab; CD3 (T cells) → T-cell lymphomas; CD19 (B cells) → ALL, target of CAR-T therapy.
🔹
CD5+/CD23+ → CLL/SLL; CD5+/CD23− → mantle cell lymphoma; CD10+ → follicular lymphoma, Burkitt lymphoma.
🔹
CD30 → Hodgkin lymphoma (Reed-Sternberg cells), anaplastic large cell lymphoma; CD15 → Hodgkin lymphoma.
🔹
Board pearl: Flow cytometry showing CD5+/CD19+/CD23+ in elderly patient with lymphocytosis → CLL.

Thyroglobulin and Differentiated Thyroid Cancer
⭐
Thyroglobulin is produced exclusively by thyroid follicular cells; after total thyroidectomy, levels should be undetectable.
⭐
Primary use: monitoring for recurrence of papillary and follicular thyroid cancer after treatment.
⭐
Anti-thyroglobulin antibodies (present in 25% of thyroid cancer patients) interfere with measurement and must be checked.
⭐
Thyroglobulin levels are most sensitive when TSH is elevated (either by thyroid hormone withdrawal or recombinant TSH).
⭐
Board distinction: Thyroglobulin for papillary/follicular cancer; calcitonin for medullary cancer; neither is useful for anaplastic cancer.

5-HIAA and Carcinoid Syndrome
✅
5-HIAA (5-hydroxyindoleacetic acid) is the urinary metabolite of serotonin, elevated in carcinoid tumors that secrete serotonin.
✅
Clinical correlation: 24-hour urine 5-HIAA is diagnostic for carcinoid syndrome (flushing, diarrhea, bronchospasm, right-sided heart disease).
✅
Only midgut carcinoids that have metastasized to liver cause carcinoid syndrome — liver normally metabolizes serotonin from portal circulation.
✅
False positives: serotonin-rich foods (bananas, avocados, walnuts) must be avoided before collection.
✅
Board pearl: Patient with flushing, diarrhea, and right-sided heart murmur → check 24-hour urine 5-HIAA for carcinoid syndrome.

Catecholamines and Pheochromocytoma
🧠
Pheochromocytomas secrete catecholamines (epinephrine, norepinephrine) causing episodic hypertension, headaches, palpitations, and diaphoresis.
🧠
Diagnostic tests: 24-hour urine or plasma fractionated metanephrines (metanephrine and normetanephrine) — more sensitive than catecholamines themselves.
🧠
Plasma free metanephrines have highest sensitivity (> 95%) but more false positives; urine metanephrines have good sensitivity with better specificity.
🧠
Interfering factors: tricyclic antidepressants, decongestants, caffeine, acetaminophen can cause false elevation.
🧠
Board clue: Young patient with paroxysmal hypertension and headaches → plasma or urine metanephrines for pheochromocytoma.

Paraproteins and Special Situations
⚡
Cryoglobulins: immunoglobulins that precipitate in cold; associated with hepatitis C, autoimmune diseases, and lymphoproliferative disorders.
⚡
Cold agglutinins: IgM antibodies causing hemolysis in cold; seen with Mycoplasma, EBV, and lymphomas.
⚡
Amyloid: misfolded proteins (often light chains in AL amyloidosis) depositing in tissues; diagnosed by Congo red staining showing apple-green birefringence.
⚡
Tumor lysis syndrome markers: rapid cancer cell death releases K⁺, phosphate, uric acid, and LDH — monitor in high-grade lymphomas and leukemias.
⚡
Board pearl: Rapid-onset renal failure with high uric acid after starting chemotherapy → tumor lysis syndrome.

Pitfalls and False Positives
📌
Benign conditions causing marker elevation: pregnancy (AFP, β-hCG, CA-125), smoking (CEA), endometriosis (CA-125), prostatitis (PSA), liver disease (many markers).
📌
Hook effect: extremely high antigen levels saturate antibodies causing falsely low results — dilute sample if suspected.
📌
Heterophile antibodies: patient antibodies against animal proteins can cause false elevation in immunoassays.
📌
Timing matters: half-life determines monitoring frequency — AFP (5 days), β-hCG (1-2 days), PSA (2-3 days), CEA (3-5 days).
📌
Board principle: Never diagnose cancer based solely on tumor marker elevation — tissue diagnosis is required.

Board Question Stem Patterns
📣
Elderly man with back pain and monoclonal spike → multiple myeloma, check calcium, creatinine, and skeletal survey.
📣
Young man with retroperitoneal mass and elevated AFP → nonseminomatous germ cell tumor.
📣
Postmenopausal woman with ascites and elevated CA-125 → suspect ovarian cancer, needs imaging and surgical evaluation.
📣
Patient with flushing, diarrhea, and elevated 5-HIAA → carcinoid syndrome, look for liver metastases.
📣
Rising CEA after colon cancer resection → recurrence, start with CT imaging.
📣
Thyroid nodule with elevated calcitonin → medullary thyroid carcinoma, screen for MEN2.
📣
Elevated PSA with low free:total ratio → increased risk of prostate cancer, consider biopsy.

One-Line Recap
🔸
Tumor markers are proteins, hormones, or metabolites produced by cancers or in response to cancer, used primarily for monitoring treatment and detecting recurrence rather than screening, with key associations including AFP (HCC, nonseminomatous germ cell tumors), CEA (colorectal cancer monitoring), CA 19-9 (pancreatic cancer), CA-125 (ovarian cancer), PSA (prostate cancer), β-hCG (gestational trophoblastic disease, germ cell tumors), and calcitonin (medullary thyroid carcinoma), remembering that no marker is perfectly sensitive or specific and tissue diagnosis remains the gold standard.

bottom of page