top of page

eduo
visual

Reproductive & Endocrine Systems
Thermogenic and Cervical Mucus Changes
Core Principle of Thermogenic and Cervical Mucus Changes
🧷
The menstrual cycle creates predictable patterns in basal body temperature (BBT) and cervical mucus consistency, both driven by the interplay between estrogen and progesterone.
🧷
These physiologic changes form the basis of fertility awareness methods and help identify ovulation timing for both conception and contraception.
🧷
Estrogen dominance in the follicular phase produces thin, clear, stretchy cervical mucus while progesterone dominance post-ovulation causes thick, opaque mucus and a sustained temperature rise.
🧷
Understanding these patterns is essential for interpreting fertility workups and counseling patients on natural family planning methods.

Hormonal Control of Basal Body Temperature
📍
BBT reflects core body temperature measured immediately upon waking, before any physical activity.
📍
During the follicular phase (pre-ovulation), BBT remains relatively low due to estrogen's slight thermogenic suppression.
📍
Progesterone, secreted by the corpus luteum after ovulation, acts on the hypothalamic thermoregulatory center → increases BBT by 0.3–0.5°C (0.5–1.0°F).
📍
This temperature rise occurs 1–2 days after ovulation and persists throughout the luteal phase.
📍
Board pearl: The sustained temperature elevation confirms that ovulation has occurred — retrospective, not predictive.

The Biphasic Temperature Pattern
🔹
A normal ovulatory cycle shows a clear biphasic pattern: lower temperatures pre-ovulation, sustained higher temperatures post-ovulation.
🔹
The temperature shift typically occurs around day 14–16 of a 28-day cycle but varies with cycle length.
🔹
If pregnancy occurs, BBT remains elevated beyond the expected luteal phase due to continued progesterone from the corpus luteum.
🔹
If no pregnancy occurs, BBT drops 1–2 days before or at the onset of menstruation as progesterone levels fall.
🔹
Board clue: Monophasic (no temperature rise) patterns indicate anovulatory cycles.

Cervical Mucus Physiology
⭐
Cervical mucus is produced by columnar epithelial cells in the endocervical canal, with composition varying dramatically across the cycle.
⭐
Mucus serves as both a barrier and a facilitator: hostile to sperm most of the month, but uniquely receptive during the fertile window.
⭐
The physical and chemical properties of mucus — hydration, pH, glycoprotein structure — are directly controlled by estrogen and progesterone levels.
⭐
Mucus evaluation provides real-time information about hormonal status, unlike BBT which confirms ovulation retrospectively.

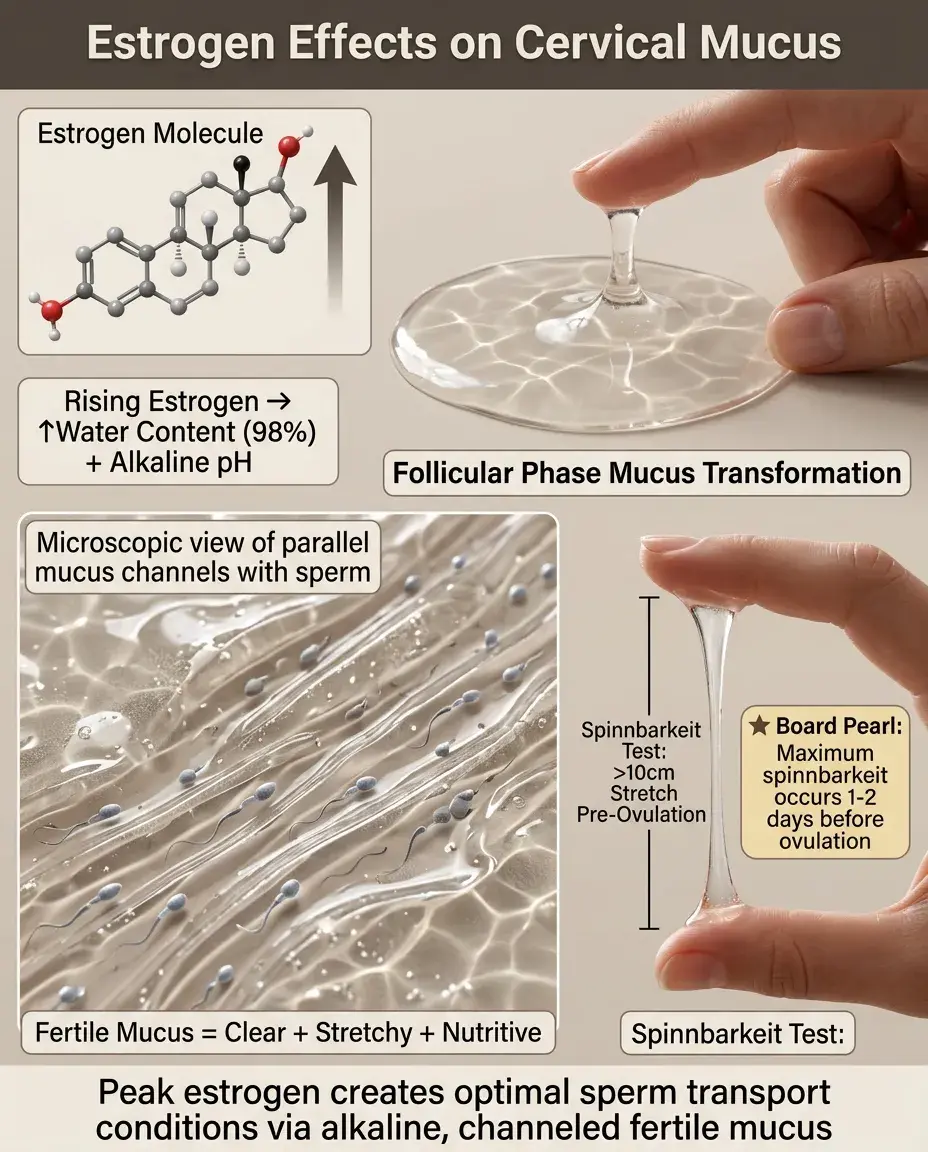
Estrogen Effects on Cervical Mucus
✅
Rising estrogen in the late follicular phase → increased mucus production, higher water content (up to 98%), alkaline pH.
✅
Peak estrogen just before ovulation produces "fertile-type" mucus: clear, slippery, stretchy (spinnbarkeit), resembling raw egg white.
✅
This mucus forms parallel channels that facilitate sperm transport, provides nutritional support, and filters out abnormal sperm.
✅
Fertile mucus can sustain sperm viability for up to 5 days in the female reproductive tract.
✅
Board pearl: Maximum stretchability (spinnbarkeit >10 cm) occurs 1–2 days before ovulation.
Progesterone Effects on Cervical Mucus
🧠
Post-ovulation progesterone → thick, opaque, sticky mucus with decreased water content and acidic pH.
🧠
This "infertile-type" mucus forms a dense network that blocks sperm penetration and creates a hostile environment.
🧠
The abrupt change from fertile to infertile mucus occurs within 24–48 hours after ovulation.
🧠
Progesterone-dominant mucus also has antimicrobial properties, protecting against ascending infections during potential early pregnancy.
🧠
Board distinction: Estrogen → quantity and quality increase; Progesterone → quantity and quality decrease.

Clinical Assessment of Cervical Mucus
⚡
Patients observe mucus at the vaginal opening or on toilet paper — no internal examination needed for fertility awareness.
⚡
Fertile mucus: clear, stretchy, slippery sensation, leaves no residue when dry.
⚡
Infertile mucus: white/yellow, tacky, sticky sensation, crumbles when dry.
⚡
The last day of fertile-type mucus correlates closely with ovulation day ("peak day").
⚡
Board pearl: Spinnbarkeit test — stretching mucus between thumb and finger; fertile mucus stretches >10 cm without breaking.

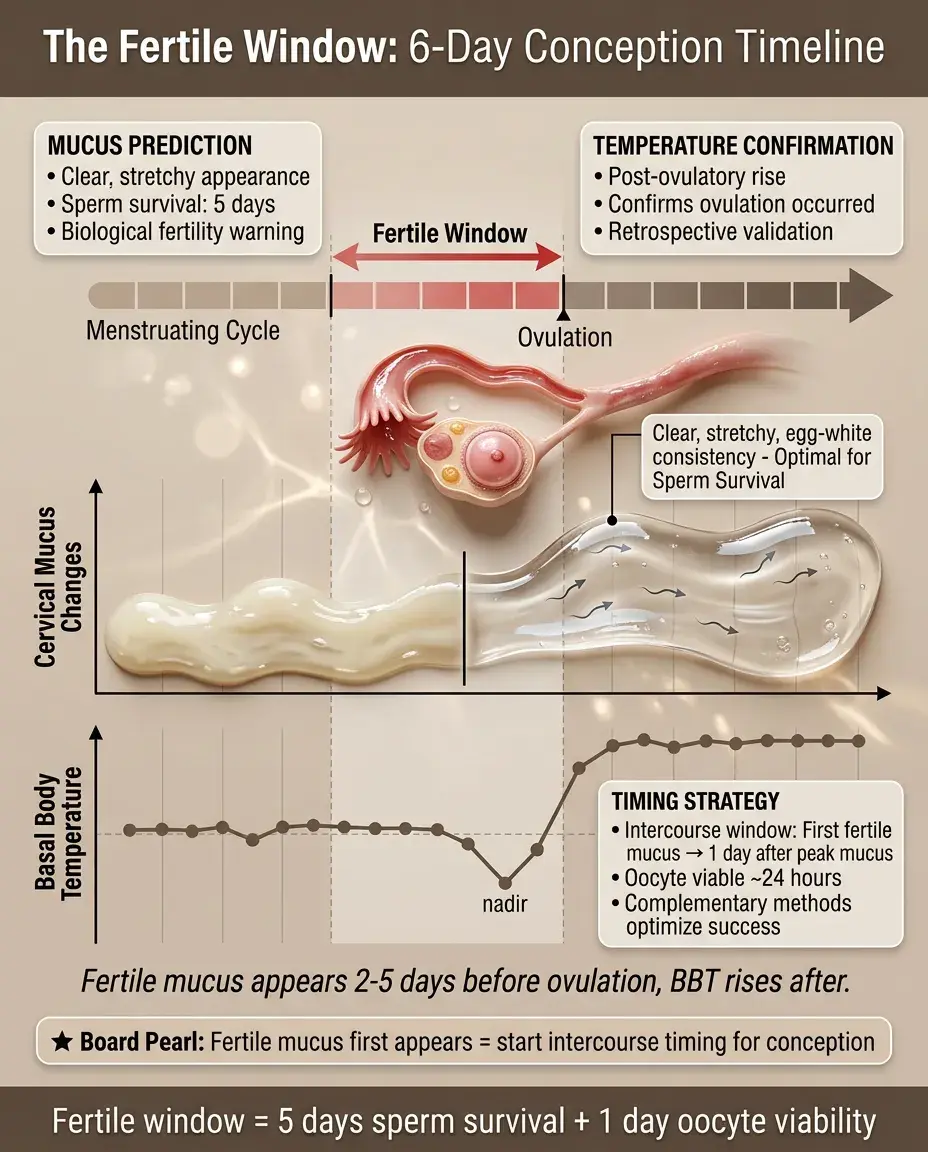
The Fertile Window Concept
📌
The fertile window spans approximately 6 days: 5 days before ovulation (sperm survival in fertile mucus) plus ovulation day (oocyte viability ~24 hours).
📌
Fertile mucus appears 2–5 days before ovulation, creating a biological warning of impending fertility.
📌
The combination of fertile mucus observation and BBT confirmation provides complementary information: mucus predicts, temperature confirms.
📌
Board clue: Questions about timing intercourse for conception → when fertile mucus first appears through 1 day after peak mucus.
Fertility Awareness Methods (FAM)
📣
FAM combines BBT charting, cervical mucus observation, and calendar calculations to identify fertile and infertile phases.
📣
Symptothermal method: uses both temperature and mucus — most effective natural method (98% with perfect use, 76% typical use).
📣
Abstinence or barrier methods required from first fertile mucus through 3 days after temperature rise.
📣
Requires daily observation, charting, and partner cooperation — not suitable for women with irregular cycles.
📣
Board distinction: FAM requires prospective daily monitoring; rhythm method uses only calendar calculations.

Clinical Applications Beyond Fertility
🔸
BBT patterns help diagnose luteal phase defects (short luteal phase <10 days or inadequate temperature rise).
🔸
Persistently monophasic BBT suggests chronic anovulation (PCOS, hypothalamic amenorrhea, hyperprolactinemia).
🔸
Cervical mucus abnormalities can indicate hormonal imbalances, cervical factor infertility, or medication effects.
🔸
Some women use mucus changes to predict menstruation or identify perimenopausal changes.
🔸
Board pearl: Clomiphene citrate paradoxically decreases cervical mucus quality despite inducing ovulation.

Factors Affecting BBT Accuracy
🧷
BBT must be measured at the same time daily, after at least 3 hours of uninterrupted sleep, before any activity.
🧷
Factors causing false elevation: fever, alcohol, sleep deprivation, sleeping late, electric blankets.
🧷
Factors causing false depression: mouth breathing, interrupted sleep, certain medications.
🧷
Shift work, travel across time zones, and irregular sleep schedules compromise BBT reliability.
🧷
Board clue: A woman with erratic BBT despite regular cycles → likely measurement error, not hormonal dysfunction.

Medications and Cervical Mucus
📍
Antihistamines and decongestants → dry all mucous membranes including cervical mucus.
📍
Clomiphene citrate → anti-estrogenic effect on cervical mucus despite stimulating ovulation.
📍
Guaifenesin (expectorant) → may improve mucus quality by increasing hydration.
📍
Hormonal contraceptives → eliminate cyclical mucus changes by suppressing ovulation.
📍
Board pearl: Discordance between ovulation induction success and pregnancy rates may indicate hostile cervical mucus.

Pathologic Cervical Mucus Patterns
🔹
Chronic thick mucus throughout cycle → cervical inflammation, infection, or scarring from procedures.
🔹
Absent mucus production → severe estrogen deficiency, cervical stenosis, congenital abnormalities.
🔹
Persistent fertile-type mucus → hyperestrogenic states, anovulatory cycles with unopposed estrogen.
🔹
Blood-tinged mucus mid-cycle → normal ovulation spotting vs. cervical pathology.
🔹
Board distinction: Post-coital test showing immotile sperm in good mucus → male factor; no sperm in mucus → cervical factor.

Special Populations and Considerations
⭐
Breastfeeding → suppresses ovulation initially, but fertile mucus returns before first postpartum ovulation.
⭐
Perimenopause → increasingly irregular patterns, more anovulatory cycles, unpredictable fertile windows.
⭐
PCOS → may have patches of fertile mucus without ovulation due to multiple follicular starts.
⭐
Post-hormonal contraception → may take several cycles for normal patterns to resume.
⭐
Board pearl: Lactational amenorrhea method (LAM) is 98% effective only if exclusively breastfeeding, amenorrheic, and <6 months postpartum.

Laboratory Correlation with Mucus and BBT
✅
Fertile mucus appearance correlates with estradiol levels >200 pg/mL.
✅
Temperature rise correlates with progesterone levels >3 ng/mL.
✅
LH surge occurs 24–36 hours before ovulation, slightly before peak mucus quality.
✅
Ultrasound confirmation: dominant follicle rupture coincides with mucus peak and precedes temperature rise.
✅
Board clue: If labs show LH surge but no temperature rise 3 days later → anovulatory LH surge (common in PCOS).

Sperm-Cervical Mucus Interaction
🧠
Fertile mucus has parallel strands creating microchannels for rapid sperm transport.
🧠
Mucus filters sperm: normal morphology and motility required to penetrate.
🧠
Alkaline pH of fertile mucus neutralizes vaginal acidity, improving sperm survival.
🧠
Capacitation begins in cervical mucus — essential for fertilization capability.
🧠
Board pearl: Post-coital test performed at mid-cycle with >10 motile sperm per HPF in clear mucus = normal.

Integration with Other Ovulation Predictors
⚡
OPKs detect LH surge → ovulation in 24–36 hours, but don't confirm ovulation occurred.
⚡
Mittelschmerz (ovulation pain) coincides with follicle rupture, occurs at mucus peak.
⚡
Cervical position changes: high/soft/open when fertile, low/firm/closed when infertile.
⚡
Combining methods increases accuracy: mucus identifies approaching ovulation, BBT confirms it occurred.
⚡
Board distinction: For contraception, the infertile phase begins only after both mucus has dried up AND temperature has been elevated for 3 days.

Common Misconceptions and Pitfalls
📌
Temperature rise does NOT predict ovulation — it confirms ovulation already occurred.
📌
Fertile mucus can appear at unexpected times in long or irregular cycles — calendar predictions unreliable.
📌
Some women never observe egg-white mucus but still have normal fertility — watery mucus is also fertile-type.
📌
Arousal fluid is not cervical mucus — it's slippery but doesn't stretch, appears only with sexual arousal.
📌
Board pearl: Stress can delay ovulation (and thus menstruation) but cannot make an established luteal phase end early.

Board Question Stem Patterns
📣
Woman charting BBT shows 18+ days of elevated temperature → pregnancy until proven otherwise.
📣
Monophasic BBT pattern in woman with regular cycles → evaluate for anovulation causes.
📣
Fertile mucus present but no temperature rise → anovulatory cycle with estrogen peak but no progesterone.
📣
Pregnancy despite avoiding intercourse after temperature rise → sperm survived in fertile mucus from earlier intercourse.
📣
Short luteal phase (<10 days of elevated BBT) → luteal phase defect, consider progesterone supplementation.
📣
Hostile post-coital test with thick mucus at mid-cycle → cervical factor infertility.

One-Line Recap
🔸
Estrogen produces clear, stretchy, fertile cervical mucus that precedes ovulation while progesterone causes thick, hostile mucus and raises basal body temperature by 0.3–0.5°C post-ovulation — patterns that together identify the fertile window for natural family planning and diagnose ovulatory dysfunction.

bottom of page