top of page

eduo
visual

Biostatistics & Epidemiology
Social and Behavioral Health Models
Core Principle of Health Behavior Models
🧷
Health behavior models provide theoretical frameworks for understanding why people engage in health-promoting or health-damaging behaviors, and how to design interventions to change behavior.
🧷
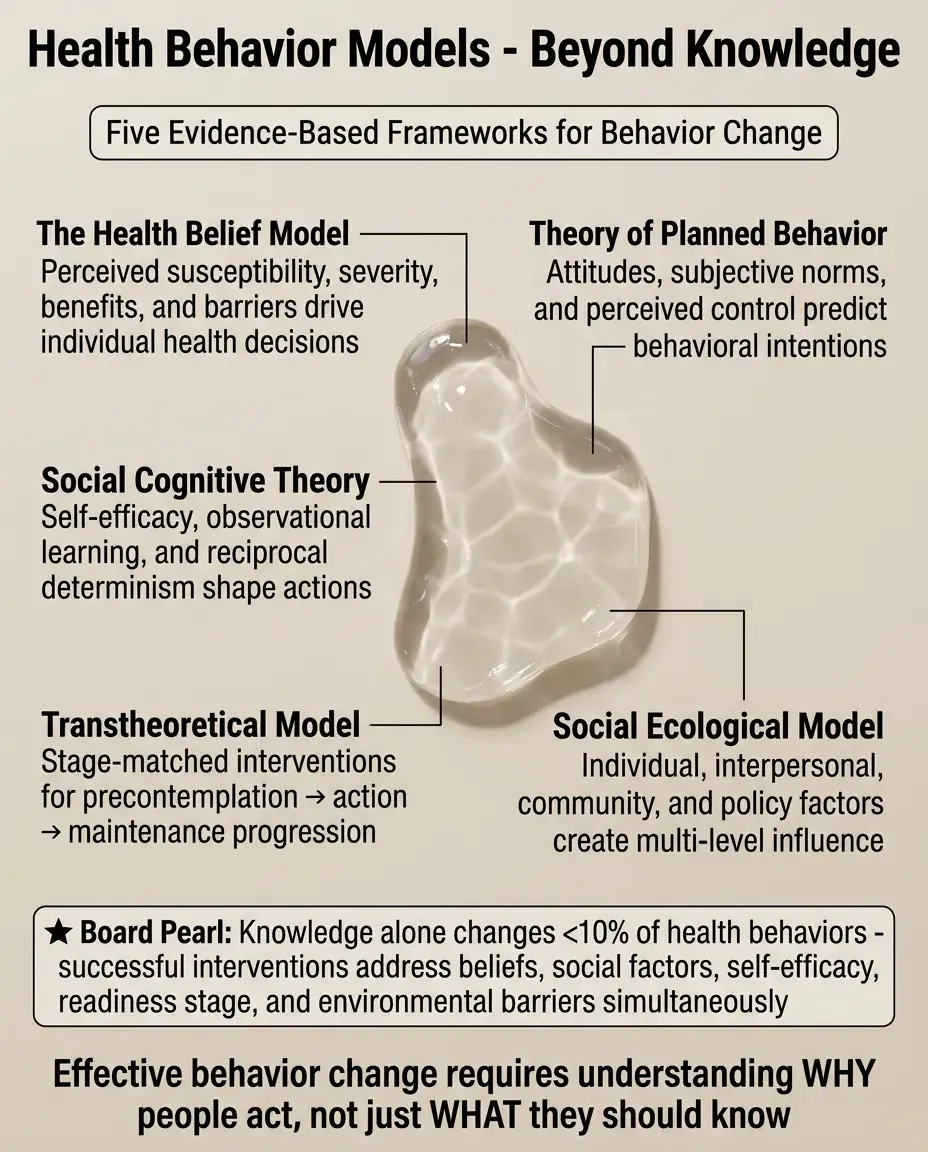
These models move beyond simple education (knowing what's healthy) to address the complex interplay of individual beliefs, social influences, and environmental factors that determine actual behavior.
🧷
Each model offers a unique lens — some focus on individual cognition, others on social networks, and others on stages of readiness to change.
🧷
Board pearl: When a question asks about designing an intervention or explaining why education alone failed, think about which behavioral model addresses the specific barrier presented.

Health Belief Model Components
📍
The Health Belief Model posits that behavior change depends on the individual's perception of four key factors: susceptibility, severity, benefits, and barriers.
📍
Perceived susceptibility: "Am I at risk?" — belief about the likelihood of getting a disease or condition.
📍
Perceived severity: "How bad would it be?" — belief about the seriousness of the condition and its consequences.
📍
Perceived benefits minus perceived barriers: "Is it worth it?" — weighing the effectiveness of the action against its costs (time, money, discomfort, inconvenience).
📍
Cues to action and self-efficacy were later additions that trigger and enable the behavior change.

Health Belief Model in Practice
🔹
A 50-year-old man won't get colonoscopy because he feels healthy (low perceived susceptibility) and thinks colon cancer is treatable if caught (low perceived severity).
🔹
Intervention must increase his perception of personal risk (family history, age-based risk) and emphasize the severity of late-stage disease.
🔹
To address barriers, provide specific information about prep tolerability, procedure time, sedation options, and insurance coverage.
🔹
Board pearl: Health Belief Model questions often present a patient who knows the recommendations but doesn't follow them — identify which perception (susceptibility, severity, benefits, barriers) needs addressing.

Theory of Planned Behavior
⭐
Behavior is determined by intention, which is influenced by three factors: attitudes toward the behavior, subjective norms, and perceived behavioral control.
⭐
Attitude: personal evaluation of the behavior as favorable or unfavorable based on expected outcomes.
⭐
Subjective norm: perception of social pressure — what important others think about the behavior and motivation to comply with their expectations.
⭐
Perceived behavioral control: belief about how easy or difficult it will be to perform the behavior, similar to self-efficacy.
⭐
Board pearl: This model uniquely emphasizes social pressure — when a question mentions peer or family influence, think Theory of Planned Behavior.

Social Cognitive Theory and Self-Efficacy
✅
Social Cognitive Theory emphasizes reciprocal determinism — the dynamic interaction between personal factors, environmental influences, and behavior, each influencing the others.
✅
Self-efficacy is the central construct: confidence in one's ability to execute behaviors necessary to produce specific performance outcomes.
✅
People learn through direct experience, observing others (modeling), and social persuasion.
✅
Environmental factors include both physical environment (access, resources) and social environment (support, norms).
✅
Board pearl: When a question emphasizes confidence or mentions learning by watching others succeed, think Social Cognitive Theory.

Transtheoretical Model Stages
🧠
Precontemplation: not considering change, may be unaware or in denial of the problem ("I don't have a drinking problem").
🧠
Contemplation: aware of the problem and considering change but ambivalent ("I know I should quit smoking, but...").
🧠
Preparation: intending to take action soon, may have taken small steps ("I bought nicotine patches").
🧠
Action: actively modifying behavior for less than 6 months ("I haven't had a cigarette in 2 months").
🧠
Maintenance: sustained behavior change for more than 6 months, working to prevent relapse.
🧠
Board pearl: Match the intervention to the stage — education for precontemplators, motivational interviewing for contemplators, specific action plans for those in preparation.

Stage-Matched Interventions
⚡
Precontemplation: raise awareness through education, personal risk assessment, and consciousness-raising activities without pressuring for immediate change.
⚡
Contemplation: explore ambivalence using motivational interviewing, weigh pros and cons, build self-efficacy, and address specific barriers.
⚡
Preparation: set specific goals, develop concrete action plans, identify resources, and anticipate challenges.
⚡
Action: provide support, teach coping skills, restructure environment, use reinforcement, and prevent early relapse.
⚡
Maintenance: focus on relapse prevention, maintain support systems, and integrate new behavior into identity.
⚡
Board pearl: A patient saying "I'm not ready to quit" is in precontemplation — pushing action-oriented strategies will fail.

Social Ecological Model Levels
📌
Individual level: knowledge, attitudes, beliefs, personality traits, and personal history that influence behavior.
📌
Interpersonal level: family, friends, peers, and social networks that provide support, role models, and social identity.
📌
Organizational level: schools, workplaces, healthcare systems with rules, regulations, and informal structures that shape behavior.
📌
Community level: neighborhoods, social norms, community resources, and networks that influence collective behavior.
📌
Policy level: local, state, and national laws and policies that regulate or support healthy behaviors.
📌
Board pearl: Effective interventions often require change at multiple levels — individual education alone rarely succeeds without environmental support.

PRECEDE-PROCEED Planning Model
📣
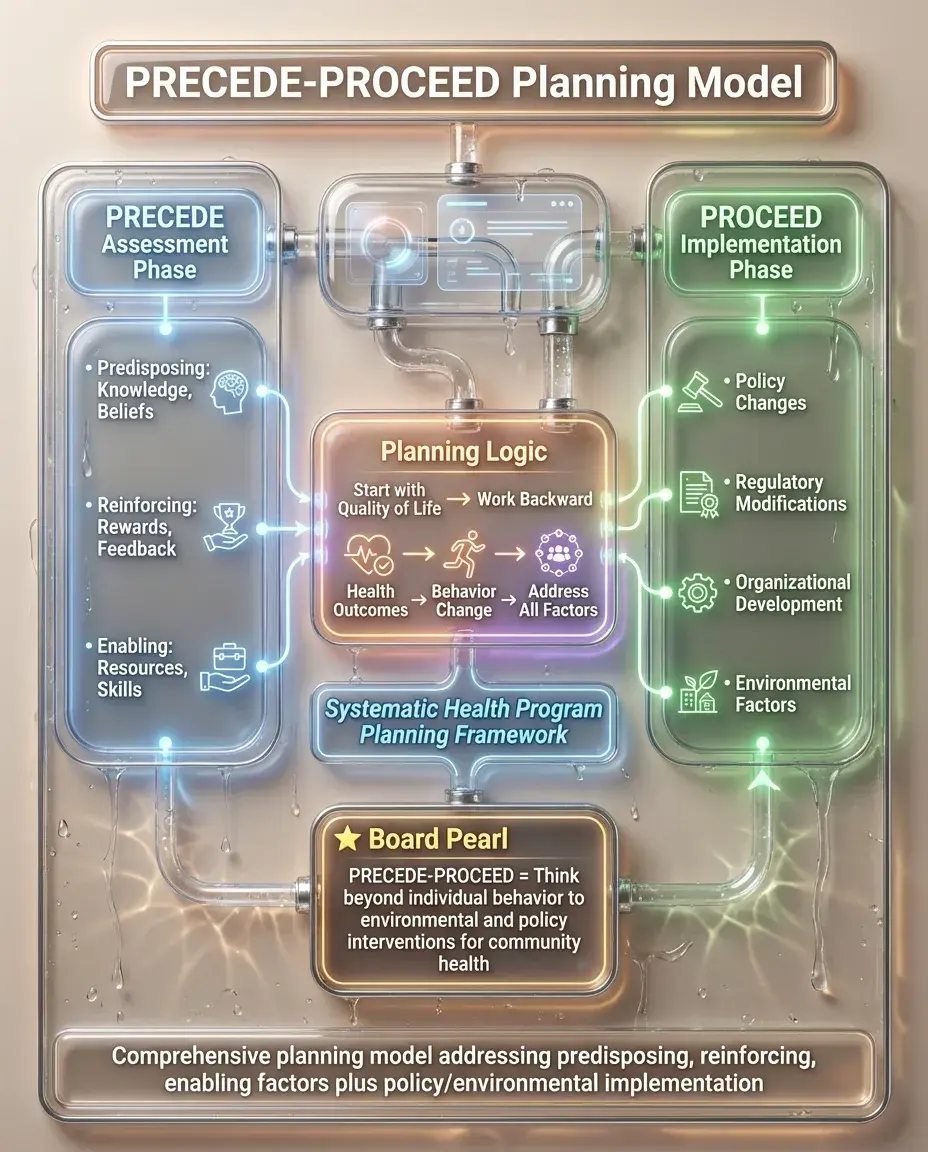
PRECEDE: Predisposing (knowledge, beliefs), Reinforcing (rewards, feedback), and Enabling (resources, skills) factors that influence behavior — assessment phase.
📣
PROCEED: Policy, Regulatory, and Organizational factors for Environmental Development — implementation and evaluation phase.
📣
This model emphasizes systematic planning: start with the desired outcome and work backward to identify all factors that must be addressed.
📣
Quality of life is the ultimate goal, achieved through health outcomes, which require behavior change, which requires addressing multiple types of factors.
📣
Board pearl: PRECEDE-PROCEED questions often ask about comprehensive community interventions — think beyond individual behavior to environmental and policy changes.
Diffusion of Innovations Theory
🔸
Describes how new ideas, behaviors, or innovations spread through a population over time via communication channels.
🔸
Adopter categories: innovators (2.5%), early adopters (13.5%), early majority (34%), late majority (34%), and laggards (16%).
🔸
Innovation characteristics that affect adoption: relative advantage, compatibility with existing values, complexity, trialability, and observability of results.
🔸
Early adopters are crucial — they're opinion leaders who influence the early and late majority.
🔸
Board pearl: When implementing a new health program, target early adopters first to create social proof and momentum for broader adoption.

Protection Motivation Theory
🧷
Focuses on how people protect themselves from health threats through two cognitive processes: threat appraisal and coping appraisal.
🧷
Threat appraisal evaluates the danger: perceived severity of the threat and perceived vulnerability to it.
🧷
Coping appraisal evaluates one's ability to cope: response efficacy (will the recommended action work?) and self-efficacy (can I do it?).
🧷
Protection motivation is highest when both threat and coping appraisals are high — people need to feel both threatened and capable of effective response.
🧷
Board pearl: Fear appeals fail when they increase threat without increasing coping ability — always pair warnings with specific, achievable action steps.

Behavioral Economics in Health
📍
Traditional models assume rational decision-making, but behavioral economics recognizes that people use mental shortcuts (heuristics) and have predictable biases.
📍
Present bias: overweighting immediate rewards versus future benefits — why people choose unhealthy foods despite knowing long-term consequences.
📍
Loss aversion: people feel losses more strongly than equivalent gains — frame messages as avoiding loss rather than achieving gain.
📍
Default bias: people tend to stick with pre-selected options — make healthy choices the default (opt-out vs. opt-in organ donation).
📍
Board pearl: Behavioral economics interventions work by changing the choice architecture rather than changing minds — nudges, not education.

Common Model Applications
🔹
Smoking cessation: Transtheoretical Model to assess readiness, Social Cognitive Theory to build self-efficacy through group programs.
🔹
Vaccine hesitancy: Health Belief Model to address low perceived susceptibility and high perceived barriers (safety concerns).
🔹
Medication adherence: Theory of Planned Behavior to address attitudes and perceived control, behavioral economics for reminder systems.
🔹
Diet and exercise: Social Ecological Model for environmental changes (workplace wellness, community resources) plus individual interventions.
🔹
Board pearl: Match the model to the specific behavioral challenge — readiness issues need stage-based approaches, social influence needs normative approaches.

Motivational Interviewing Principles
⭐
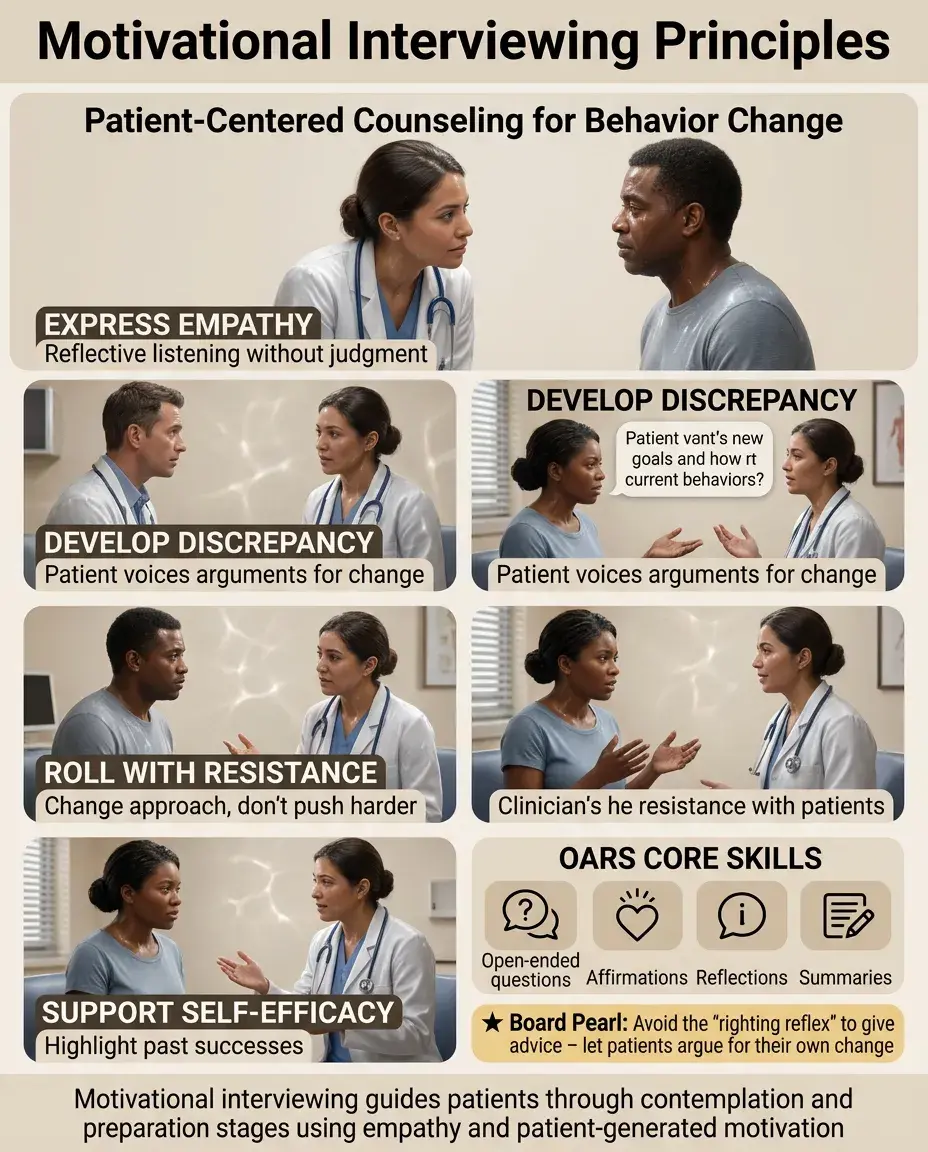
A counseling approach aligned with the Transtheoretical Model, especially useful in contemplation and preparation stages.
⭐
Express empathy through reflective listening — understand the patient's perspective without judgment.
⭐
Develop discrepancy between current behavior and personal values or goals — let the patient voice the arguments for change.
⭐
Roll with resistance rather than confronting it directly — resistance is a signal to change approach, not push harder.
⭐
Support self-efficacy by highlighting past successes and building confidence in ability to change.
⭐
Board pearl: Open-ended questions, affirmations, reflections, and summaries (OARS) are the core skills — avoid the "righting reflex" to give advice.
Cultural Considerations in Health Behavior
✅
Cultural values profoundly influence health beliefs, perceived social norms, and acceptable behavior change strategies.
✅
Collectivist cultures may respond better to interventions emphasizing family or community benefit versus individual benefit.
✅
Fatalistic beliefs ("It's in God's hands") require different approaches than those emphasizing personal control.
✅
Language barriers affect not just communication but conceptual understanding — "depression" may not translate conceptually across cultures.
✅
Board pearl: Effective interventions must be culturally adapted, not just translated — involve community members in design and implementation.

Implementation Science and Model Integration
🧠
Real-world interventions often combine multiple models to address different aspects of behavior change.
🧠
The RE-AIM framework evaluates interventions: Reach (who participates), Effectiveness (outcomes), Adoption (by organizations), Implementation (fidelity), and Maintenance (sustainability).
🧠
Process evaluation is as important as outcome evaluation — understanding why an intervention worked or failed.
🧠
Context matters: an intervention effective in one setting may fail in another due to different barriers, resources, or cultural factors.
🧠
Board pearl: Board questions about failed interventions often hinge on implementation problems — right model, wrong application or context.

Technology and Digital Health Behavior Change
⚡
Digital interventions can deliver model-based behavior change at scale: apps for self-monitoring, SMS reminders, online social support.
⚡
Gamification applies behavioral economics principles: immediate rewards, progress tracking, social comparison, and achievement levels.
⚡
Just-in-time adaptive interventions use sensors and algorithms to deliver support at moments of greatest need or receptivity.
⚡
Digital divide concerns: interventions may widen health disparities if they require technology access or digital literacy.
⚡
Board pearl: Technology amplifies model-based interventions but doesn't replace the need for behavior change theory — the medium is not the message.

Common Pitfalls in Behavior Change
📌
Information-behavior gap: assuming education alone will change behavior ignores emotional, social, and environmental factors.
📌
One-size-fits-all approaches: failing to match intervention to stage of change, cultural context, or specific barriers.
📌
Individual blame: focusing only on personal responsibility while ignoring environmental and policy factors that constrain choices.
📌
Short-term thinking: expecting immediate results when behavior change is a process requiring sustained support.
📌
Board pearl: When a board question describes an intervention failure, look for these pitfalls — especially mismatch between intervention and behavioral determinants.

Board Question Stem Patterns
📣
Patient knows smoking is harmful but continues → assess stage of change before recommending specific interventions.
📣
Community program to increase exercise fails despite education → consider environmental barriers and social ecological factors.
📣
Teenager won't use contraception despite sex education → explore subjective norms and perceived behavioral control.
📣
Elderly patient non-adherent to medications → assess specific barriers (cost, complexity, beliefs about necessity).
📣
Fear-based campaign increases anxiety but not behavior change → add coping strategies and self-efficacy building.
📣
Cultural community has low vaccination rates → engage community leaders, address cultural beliefs, use appropriate models.

One-Line Recap
🔸
Health behavior models explain why knowledge alone rarely changes behavior by addressing individual beliefs (Health Belief Model), social influences (Theory of Planned Behavior), self-efficacy (Social Cognitive Theory), readiness to change (Transtheoretical Model), and environmental factors (Social Ecological Model), guiding stage-matched, culturally appropriate, multi-level interventions that recognize both rational and irrational decision-making processes.
bottom of page