top of page

eduo
visual

Behavioral Health & Nervous System
Sleep Disorders: Insomnia, Narcolepsy, Parasomnias, Sleep Apnea
Core Principle of Sleep Architecture and Disorders
🧷
Sleep follows a predictable architecture: NREM stages 1-3 (progressively deeper sleep) → REM sleep, cycling every 90-120 minutes.
🧷
Sleep disorders disrupt either the initiation/maintenance of sleep (insomnia, sleep apnea), the timing of sleep-wake cycles (circadian rhythm disorders), or produce abnormal behaviors during sleep (parasomnias).
🧷
The key to board questions is recognizing the pathophysiology: respiratory obstruction, loss of orexin neurons, dopaminergic dysfunction, or primary CNS arousal dysregulation.
🧷
Sleep complaints are among the most common in medicine, but distinguishing primary sleep disorders from sleep disruption secondary to medical/psychiatric conditions is essential.

Insomnia: Definition and Classification
📍
Insomnia is difficulty initiating sleep (>30 minutes), maintaining sleep (frequent awakenings), or early morning awakening with inability to return to sleep, occurring ≥3 nights/week for ≥3 months.
📍
Primary insomnia occurs without identifiable medical, psychiatric, or substance-related cause.
📍
Secondary insomnia is far more common: depression, anxiety, pain, medications (steroids, stimulants), substances (caffeine, alcohol withdrawal), or medical conditions (hyperthyroidism, GERD).
📍
Board pearl: Insomnia with early morning awakening is a classic feature of major depression; insomnia with difficulty initiating sleep suggests anxiety.

Sleep Hygiene and Behavioral Interventions
🔹
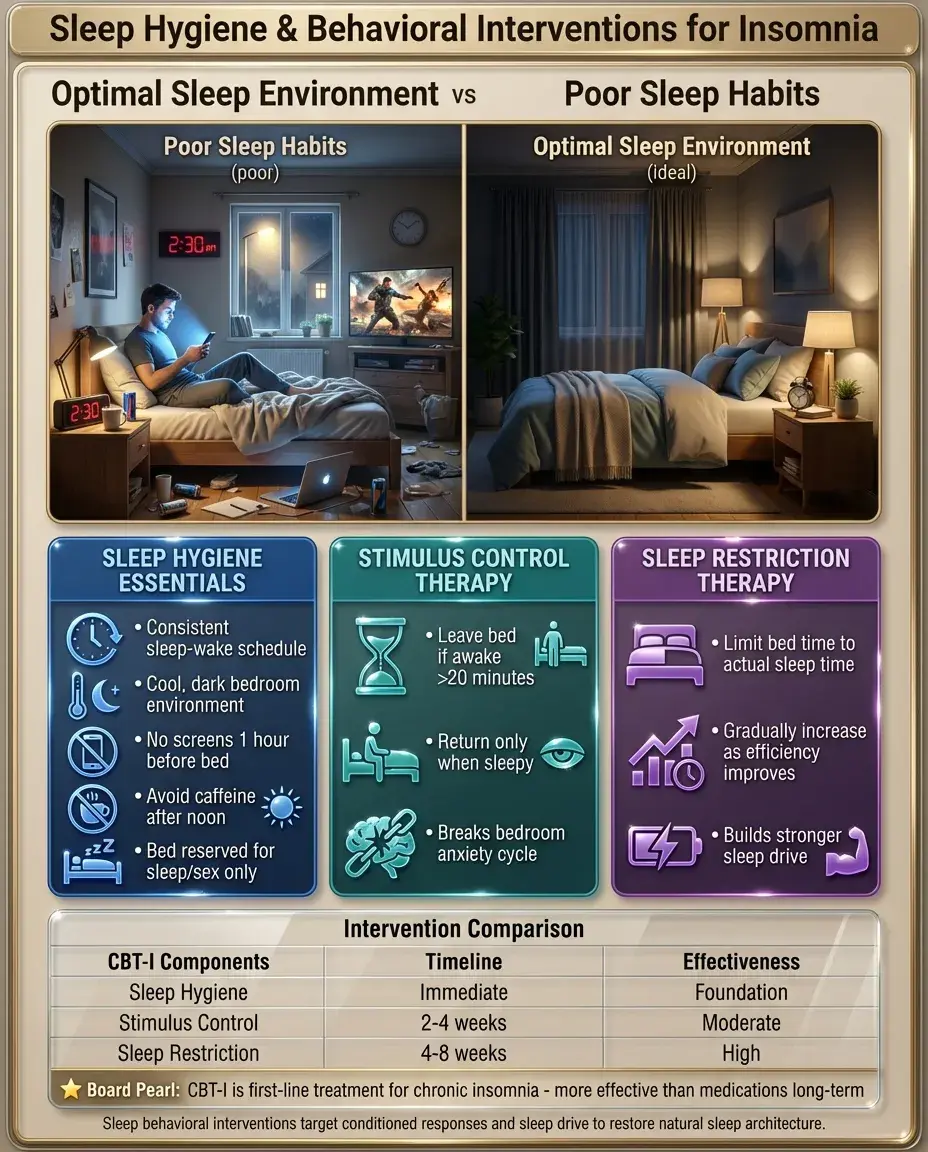
Sleep hygiene includes consistent sleep-wake times, avoiding screens before bed, cool dark room, avoiding caffeine after noon, and reserving bed for sleep and sex only.
🔹
Stimulus control therapy: leave bed if unable to sleep within 20 minutes, return only when sleepy — breaks the conditioned anxiety response to the bedroom.
🔹
Sleep restriction therapy: limit time in bed to actual sleep time, then gradually increase as sleep efficiency improves.
🔹
Board pearl: Cognitive behavioral therapy for insomnia (CBT-I) is first-line treatment for chronic insomnia, more effective than medications long-term.
Narcolepsy: Loss of Orexin Signaling
⭐
Narcolepsy type 1 results from autoimmune destruction of orexin (hypocretin)-producing neurons in the lateral hypothalamus, leading to unstable transitions between wake and sleep states.
⭐
The tetrad: excessive daytime sleepiness, cataplexy (sudden bilateral muscle atonia triggered by emotions), hypnagogic/hypnopompic hallucinations, and sleep paralysis.
⭐
Cataplexy is pathognomonic for narcolepsy type 1 — conscious drop attacks triggered by laughter, surprise, or anger.
⭐
Narcolepsy type 2 lacks cataplexy and has normal orexin levels, suggesting a different pathophysiology.
⭐
Board pearl: Low CSF orexin (<110 pg/mL) is diagnostic for narcolepsy type 1.

Multiple Sleep Latency Test and REM Intrusions
✅
The MSLT is the gold standard for diagnosing narcolepsy: 5 scheduled naps across the day, measuring time to sleep onset and REM latency.
✅
Narcolepsy shows mean sleep latency <8 minutes (often <5 minutes) and ≥2 sleep-onset REM periods (SOREMPs).
✅
Normal individuals take 15-20 minutes to fall asleep and 90 minutes to enter REM; narcolepsy patients enter REM within minutes.
✅
The pathophysiology explains the symptoms: REM atonia intrudes into wakefulness (cataplexy), REM dreams intrude into wake-sleep transitions (hallucinations), and REM atonia persists on awakening (sleep paralysis).

Obstructive Sleep Apnea: Upper Airway Collapse
🧠
OSA results from repetitive pharyngeal collapse during sleep → apnea/hypopnea → hypoxemia and arousal → sleep fragmentation.
🧠
Risk factors follow from anatomy and physics: obesity (pharyngeal fat deposition), large neck circumference (>17" men, >16" women), retrognathia, macroglossia, tonsillar hypertrophy.
🧠
The classic triad: loud snoring, witnessed apneas, and excessive daytime sleepiness.
🧠
Apnea-hypopnea index (AHI) defines severity: mild 5-15, moderate 15-30, severe >30 events/hour.
🧠
Board pearl: OSA is associated with resistant hypertension, atrial fibrillation, and increased cardiovascular mortality.

Pathophysiology and Complications of OSA
⚡
Repeated hypoxia-reoxygenation cycles → oxidative stress → endothelial dysfunction → atherosclerosis acceleration.
⚡
Intrathoracic pressure swings → increased LV afterload and atrial stretch → atrial fibrillation.
⚡
Hypoxemia and hypercapnia → pulmonary vasoconstriction → pulmonary hypertension → right heart strain.
⚡
Sleep fragmentation → sympathetic activation → resistant hypertension (especially loss of nocturnal dipping).
⚡
Board pearl: Morning headaches in OSA result from nocturnal CO₂ retention causing cerebral vasodilation.

Central Sleep Apnea and Cheyne-Stokes Respiration
📌
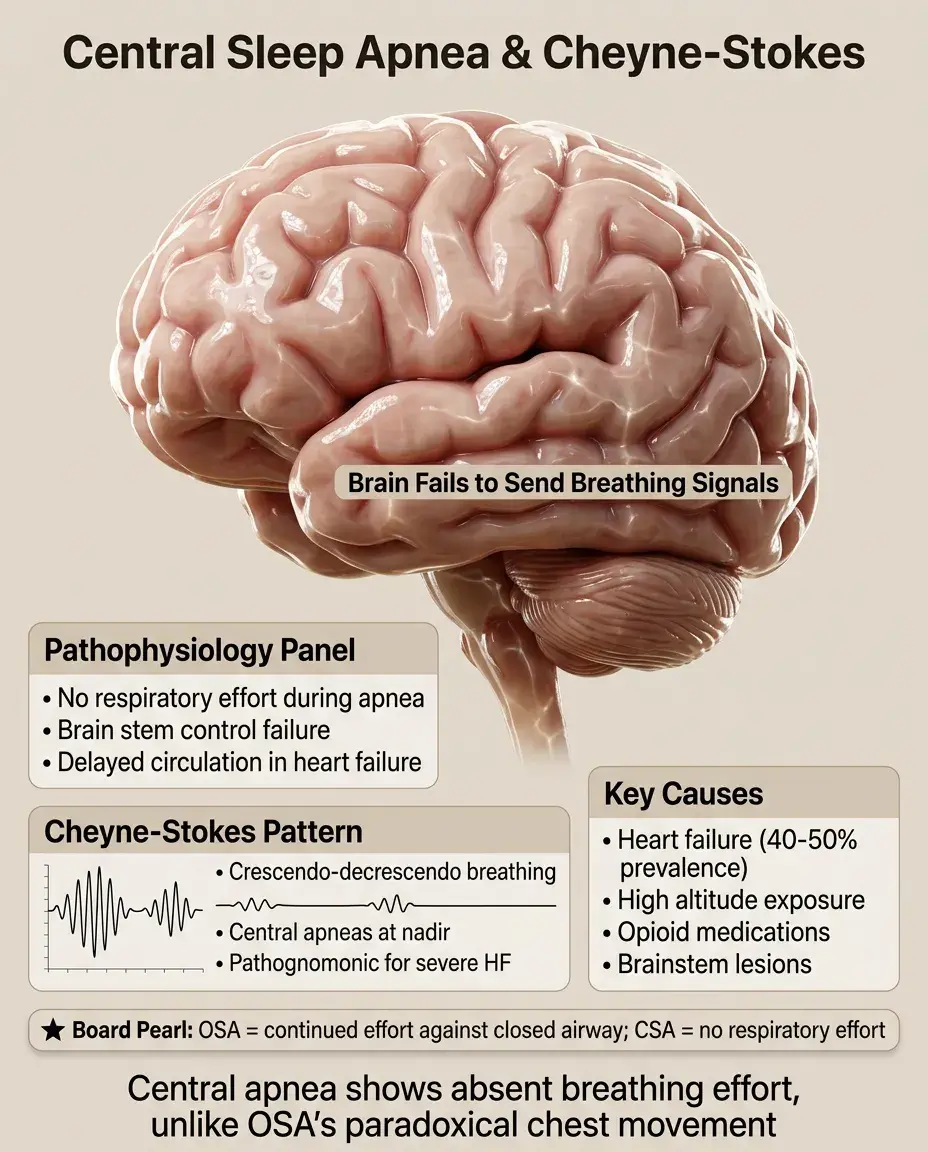
Central sleep apnea lacks respiratory effort during apneas — the brain fails to send breathing signals.
📌
Most common in heart failure (40-50% prevalence), where delayed circulation time causes unstable ventilatory control.
📌
Cheyne-Stokes respiration: crescendo-decrescendo breathing pattern with central apneas at the nadir, pathognomonic for severe heart failure.
📌
High altitude, opioids, and brainstem lesions are other causes of central apnea.
📌
Board distinction: OSA shows continued respiratory effort against closed airway (paradoxical chest-abdomen movement); CSA shows absent effort.
NREM Parasomnias: Disorders of Arousal
📣
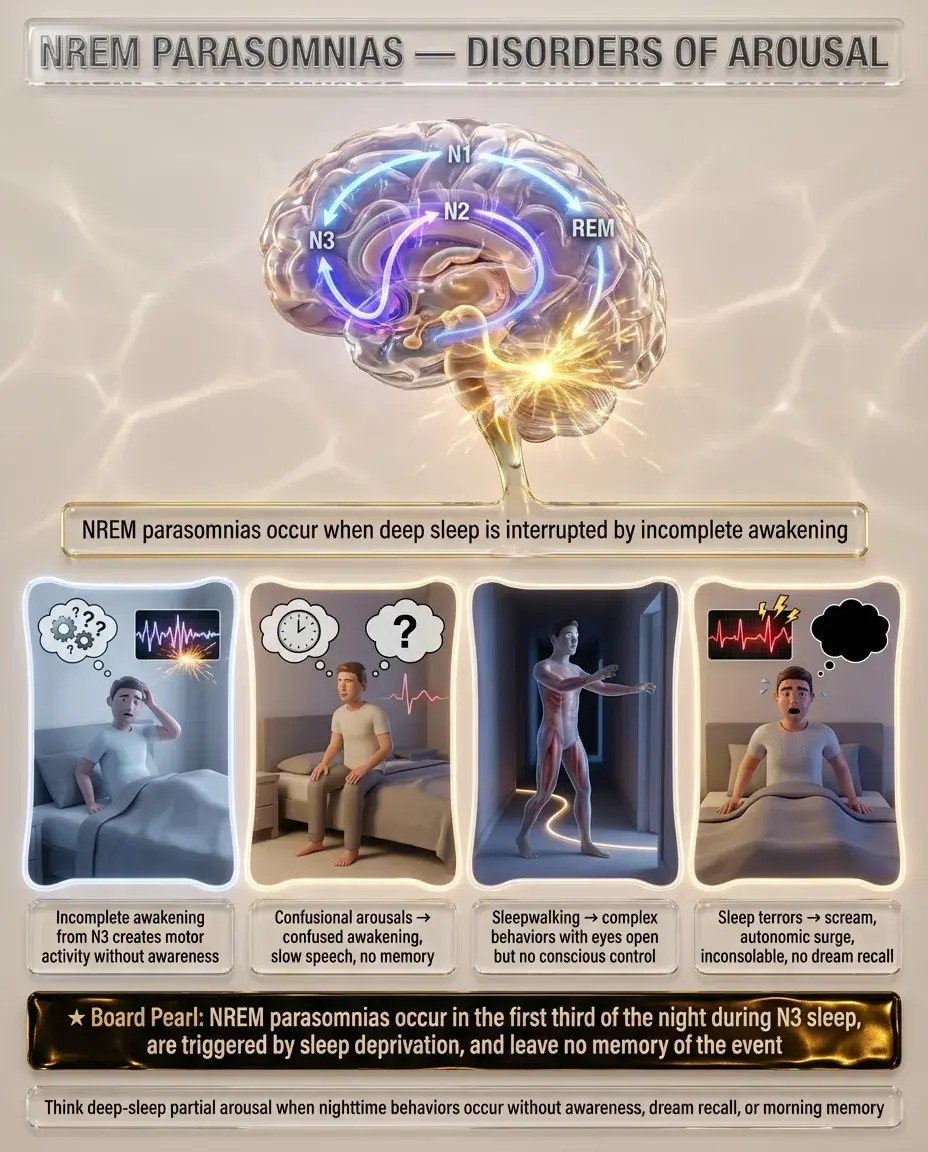
NREM parasomnias arise from incomplete awakening from deep sleep (N3), creating a dissociated state with motor activity but no conscious awareness.
📣
Confusional arousals: sitting up confused, slow speech, inappropriate responses, no memory of event.
📣
Sleepwalking: complex motor behaviors (walking, eating, even driving) with eyes open but no conscious control.
📣
Sleep terrors: sudden arousal with piercing scream, autonomic activation, inconsolable, no dream recall.
📣
Board pearl: NREM parasomnias occur in the first third of night when N3 predominates, have amnesia for events, and are triggered by sleep deprivation.
REM Sleep Behavior Disorder: Loss of REM Atonia
🔸
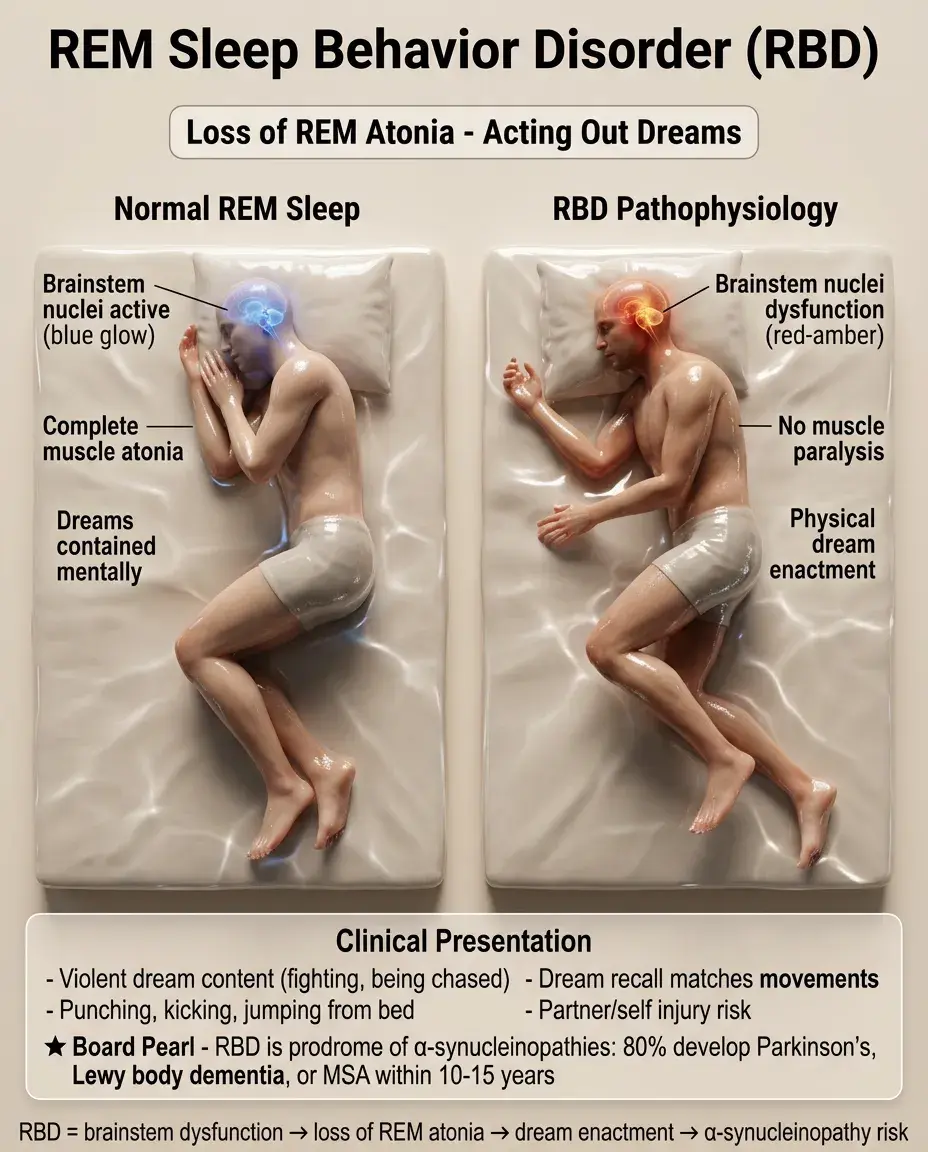
RBD results from dysfunction of brainstem nuclei that normally induce muscle atonia during REM sleep.
🔸
Patients literally act out their dreams — punching, kicking, jumping out of bed — often injuring themselves or bed partners.
🔸
Dreams are typically violent or action-filled (being chased, fighting attackers), and patients can recall dream content that matches their movements.
🔸
Board pearl: RBD is a prodrome of α-synucleinopathies — 80% develop Parkinson disease, dementia with Lewy bodies, or multiple system atrophy within 10-15 years.
Circadian Rhythm Sleep-Wake Disorders
🧷
Delayed sleep-wake phase disorder: intrinsic circadian clock runs late → cannot fall asleep until 2-6 AM, extreme difficulty waking for school/work.
🧷
Advanced sleep-wake phase disorder: early sleep onset (6-8 PM) and early awakening (2-4 AM), more common in elderly.
🧷
Non-24-hour sleep-wake rhythm disorder: circadian period >24 hours → progressively later sleep times each day, classic in blind individuals lacking light entrainment.
🧷
Shift work disorder: misalignment between work schedule and circadian rhythm → insomnia during desired sleep time and sleepiness during work.

Restless Legs Syndrome and Periodic Limb Movements
📍
RLS is a sensorimotor disorder with four essential criteria: urge to move legs, worse at rest, relieved by movement, worse in evening/night.
📍
Patients describe crawling, pulling, or electric sensations deep in legs — not surface paresthesias.
📍
Strong association with iron deficiency (ferritin <50-75 μg/L), pregnancy, uremia, and neuropathy.
📍
Periodic limb movements of sleep (PLMS): repetitive dorsiflexion of ankle/big toe every 20-40 seconds, may occur with or without RLS.
📍
Board pearl: Dopamine agonists are first-line for moderate-severe RLS; iron supplementation if ferritin <75.

Kleine-Levin Syndrome and Hypersomnia Disorders
🔹
Kleine-Levin syndrome: episodic hypersomnia (sleeping 16-20 hours/day) with cognitive dysfunction, derealization, and often hyperphagia and hypersexuality during episodes.
🔹
Episodes last days to weeks, with complete normalcy between episodes — affects adolescent males predominantly.
🔹
Idiopathic hypersomnia: chronic excessive sleep (>10 hours/night) with severe sleep inertia despite adequate sleep duration.
🔹
Post-infectious hypersomnia can follow viral infections, suggesting autoimmune etiology.
🔹
Board distinction: Narcolepsy has short refreshing naps; idiopathic hypersomnia has long unrefreshing sleep.

Sleep-Related Movement Disorders
⭐
Rhythmic movement disorder: head banging, body rocking, or leg rolling at sleep onset — normal in infants, concerning if persists past age 5.
⭐
Sleep starts (hypnic jerks): sudden muscle contractions at sleep onset, universal and benign.
⭐
Propriospinal myoclonus: jerks originating in spinal cord at sleep-wake transition.
⭐
Bruxism: teeth grinding during sleep → dental wear, jaw pain, headaches; associated with stress and SSRIs.
⭐
Board pearl: Nocturnal leg cramps (charley horses) are painful sustained contractions, distinct from RLS or PLMS.

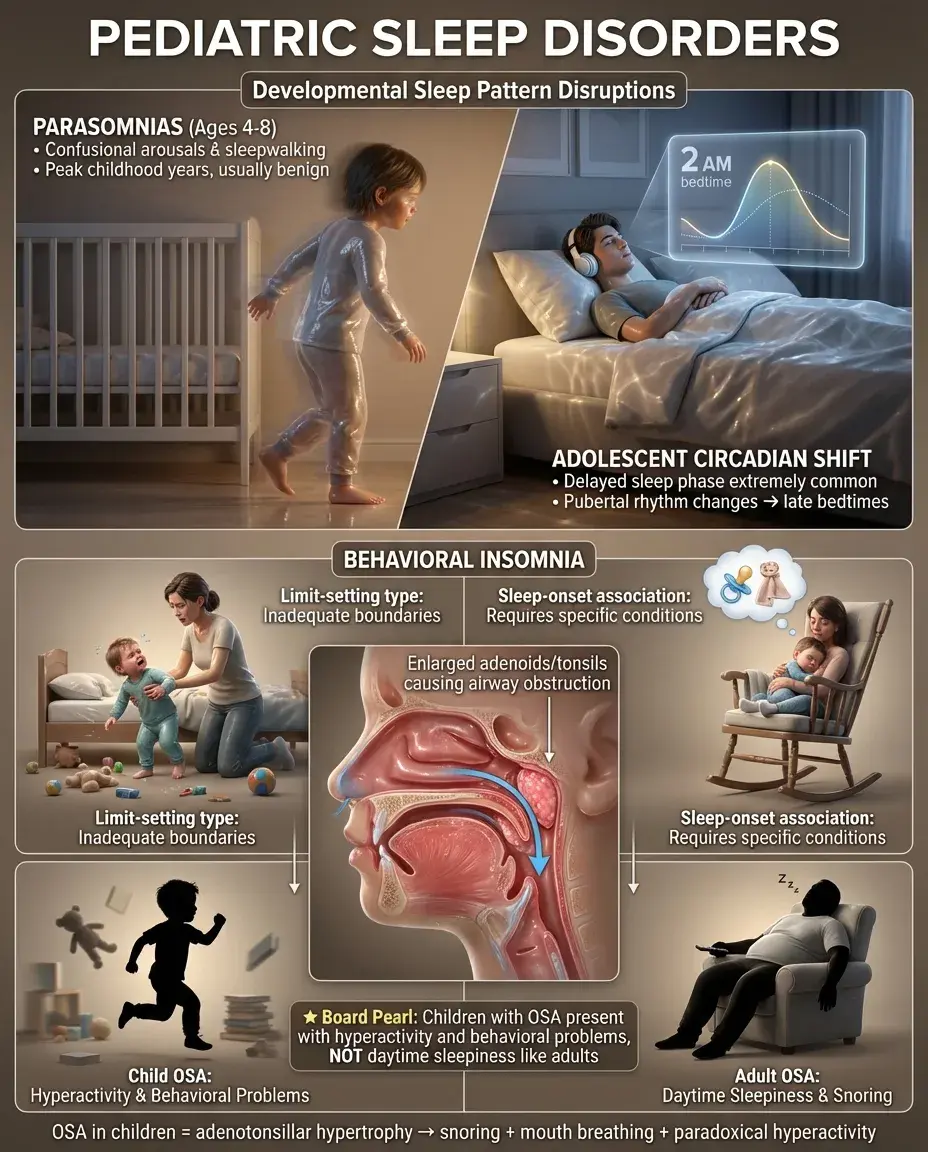
Pediatric Sleep Disorders
✅
Behavioral insomnia of childhood: limit-setting type (inadequate boundaries) vs sleep-onset association type (requires specific conditions to fall asleep).
✅
Confusional arousals and sleepwalking peak at ages 4-8 years, usually benign and outgrown.
✅
Delayed sleep phase is extremely common in adolescents due to pubertal shift in circadian rhythm.
✅
Obstructive sleep apnea in children usually results from adenotonsillar hypertrophy — presents as snoring, mouth breathing, and paradoxically hyperactivity rather than sleepiness.
✅
Board pearl: Unlike adults, children with OSA often present with behavioral problems and poor school performance rather than daytime sleepiness.
Sleep Disorders in Medical Conditions
🧠
Parkinson disease: REM behavior disorder (early), fragmented sleep, restless legs syndrome.
🧠
Alzheimer disease: sundowning, fragmented sleep-wake cycles, eventual complete circadian disruption.
🧠
Depression: early morning awakening, decreased REM latency, increased REM density.
🧠
Chronic pain syndromes: alpha wave intrusions into deep sleep, nonrestorative sleep.
🧠
GERD: nocturnal reflux causes arousals, worse in first half of night when supine.
🧠
Board pearl: Nocturnal panic attacks occur during NREM sleep; nightmares occur during REM sleep.

Medications Affecting Sleep
⚡
Medications causing insomnia: stimulants, steroids, beta-blockers (nightmares), SSRIs (REM suppression), decongestants, thyroid hormone.
⚡
Medications causing daytime sleepiness: antihistamines, benzodiazepines, opioids, muscle relaxants, antipsychotics.
⚡
REM suppressants: SSRIs, SNRIs, TCAs, MAOIs — abrupt discontinuation can cause REM rebound with vivid dreams.
⚡
Medications triggering RLS: antihistamines, antidepressants (except bupropion), antipsychotics, antiemetics.
⚡
Board pearl: Beta-blockers cause nightmares by allowing melatonin suppression; prazosin reduces nightmares in PTSD.

Diagnostic Testing in Sleep Medicine
📌
Polysomnography records EEG, EOG, EMG, ECG, respiratory effort, airflow, oxygen saturation, and limb movements.
📌
Home sleep apnea testing measures airflow, respiratory effort, and oxygen saturation — adequate for uncomplicated OSA but cannot diagnose other sleep disorders.
📌
Actigraphy uses wrist-worn accelerometer to estimate sleep-wake patterns over weeks — useful for circadian rhythm disorders.
📌
Maintenance of Wakefulness Test assesses ability to stay awake — required for commercial drivers treated for OSA.
📌
Board pearl: PSG is required for suspected narcolepsy, parasomnias, or when home testing is negative despite high clinical suspicion.

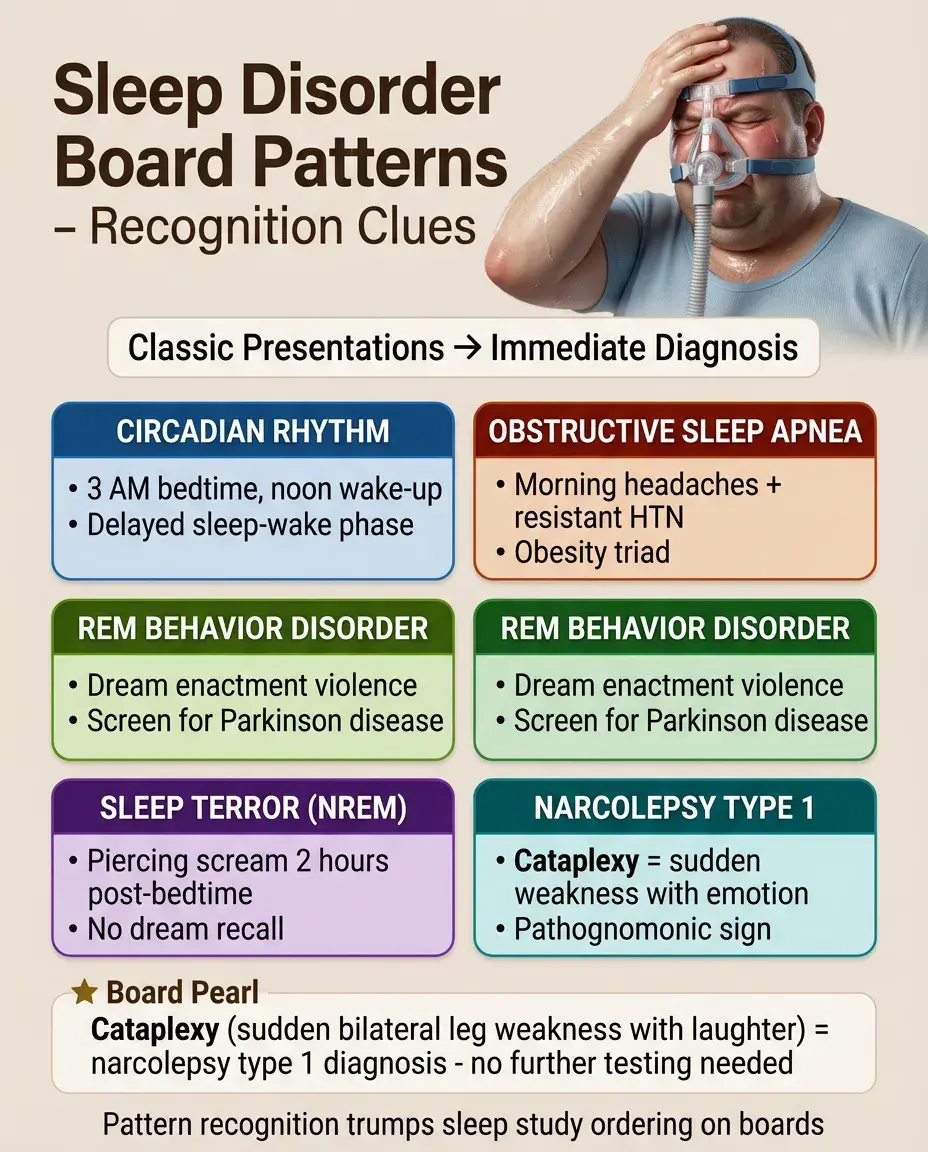
Board Question Stem Patterns
📣
Teenager unable to fall asleep until 3 AM, sleeps until noon on weekends → delayed sleep-wake phase disorder.
📣
Obese patient with morning headaches and resistant hypertension → obstructive sleep apnea.
📣
Patient punching spouse while dreaming of fighting → REM behavior disorder, screen for Parkinson disease.
📣
Child with piercing scream 2 hours after bedtime, no recall → sleep terror (NREM parasomnia).
📣
Sudden bilateral leg weakness triggered by laughter → cataplexy, diagnostic of narcolepsy type 1.
📣
Heart failure patient with crescendo-decrescendo breathing → Cheyne-Stokes respiration.
📣
Urge to move legs worse at night, relieved by walking → restless legs syndrome, check ferritin.
One-Line Recap
🔸
Sleep disorders encompass disrupted sleep architecture from airway obstruction (OSA), orexin loss (narcolepsy), incomplete NREM arousal (parasomnias), failed REM atonia (RBD), circadian misalignment, and iron/dopamine dysfunction (RLS), each with distinct pathophysiology, diagnostic testing (PSG, MSLT), and treatment implications ranging from CPAP to dopamine agonists to behavioral interventions.

bottom of page