top of page

eduo
visual

Behavioral Health & Nervous System
Sleep Architecture: REM and NREM Stages
Core Principle of Sleep Architecture
🧷
Sleep is an active neurobiological process organized into two distinct states: rapid eye movement (REM) sleep and non-rapid eye movement (NREM) sleep, cycling predictably throughout the night.
🧷
NREM sleep is further divided into three stages (N1, N2, N3), each with characteristic EEG patterns, physiological changes, and functions.
🧷
A typical night consists of 4–6 cycles of NREM→REM progression, each lasting approximately 90–120 minutes, with deeper NREM sleep dominating early cycles and REM sleep increasing in duration and density toward morning.
🧷
Understanding sleep architecture is essential for recognizing how medications, medical conditions, and sleep disorders disrupt normal restorative processes.

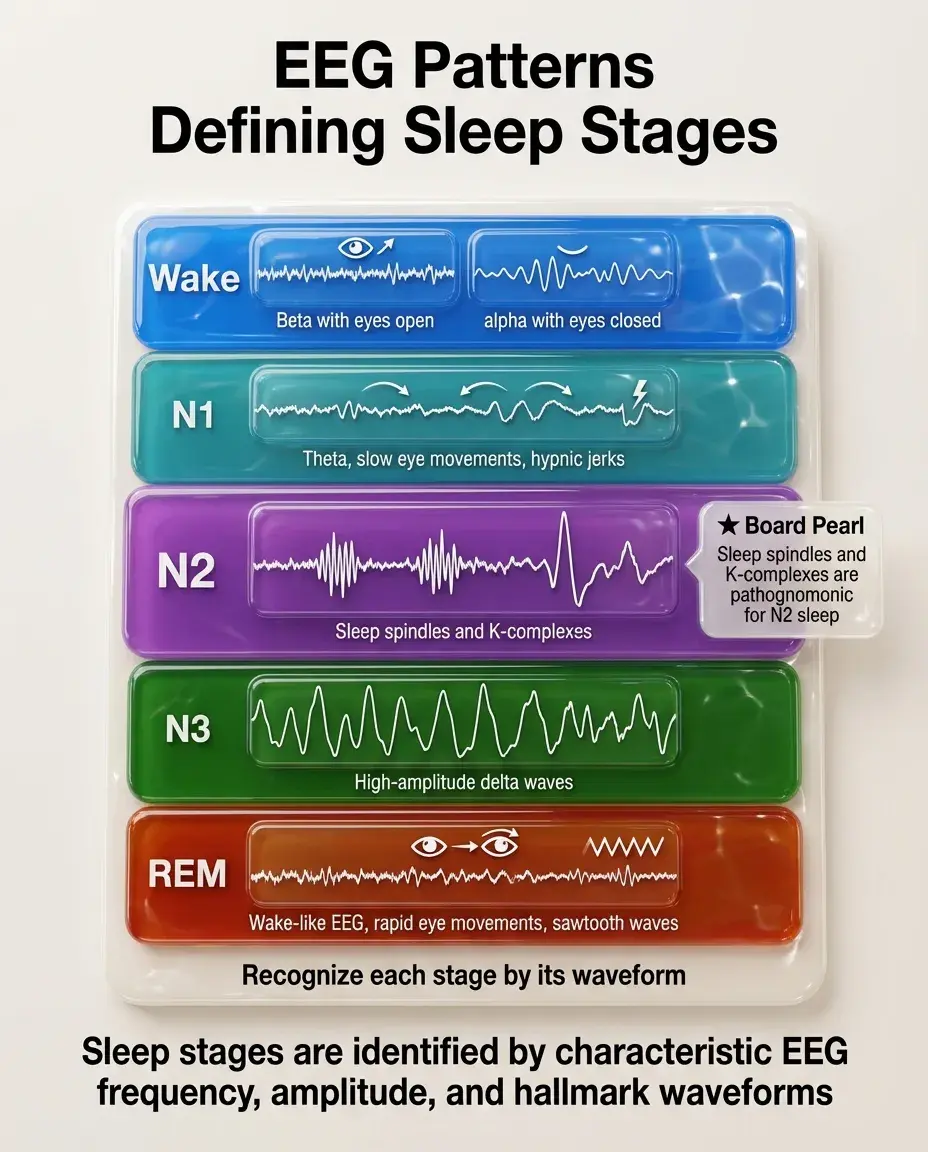
EEG Patterns Defining Sleep Stages
📍
Wake: low-amplitude, high-frequency beta waves (13–30 Hz) with eyes open; alpha waves (8–12 Hz) with eyes closed.
📍
N1 (light sleep): theta waves (4–7 Hz), vertex sharp waves, slow rolling eye movements, hypnic jerks.
📍
N2 (intermediate sleep): background theta with sleep spindles (12–14 Hz bursts) and K-complexes (large biphasic waves).
📍
N3 (deep/slow-wave sleep): high-amplitude delta waves (0.5–4 Hz) comprising >20% of epoch.
📍
REM: low-amplitude, mixed-frequency waves resembling wake EEG, rapid eye movements, sawtooth waves.
📍
Board pearl: Sleep spindles and K-complexes are pathognomonic for N2 sleep.
NREM Sleep Physiology and Functions
🔹
NREM sleep is characterized by synchronized cortical activity, decreased muscle tone (but not atonia), decreased temperature, heart rate, and blood pressure.
🔹
N3 (slow-wave sleep) is the deepest stage, with highest arousal threshold and most restorative functions.
🔹
Growth hormone secretion peaks during N3, making it critical for physical recovery, tissue repair, and growth.
🔹
Memory consolidation during NREM focuses on declarative memory (facts and events) through hippocampal-neocortical dialogue.
🔹
Board pearl: Night terrors, sleepwalking, and confusional arousals occur during N3 sleep, not REM sleep.

REM Sleep Physiology and Characteristics
⭐
REM sleep features cortical activation with complete skeletal muscle atonia (except diaphragm and extraocular muscles), preventing dream enactment.
⭐
Autonomic instability: fluctuating heart rate, blood pressure, temperature regulation impaired, penile erections/clitoral engorgement.
⭐
Vivid, complex, emotionally intense dreams with bizarre content and narrative structure.
⭐
Accounts for 20–25% of total sleep time in adults, occurring in longer, more intense periods toward morning.
⭐
Board pearl: REM sleep behavior disorder results from loss of normal REM atonia, allowing patients to physically act out dreams.

Sleep Cycle Progression Through the Night
✅
First cycle: Wake → N1 → N2 → N3 → N2 → brief REM (5–10 minutes).
✅
Early cycles (first half of night): dominated by N3 slow-wave sleep, minimal REM.
✅
Later cycles (second half of night): N3 decreases or disappears, REM periods lengthen to 20–40 minutes.
✅
Total sleep architecture: N1 (5%), N2 (45–55%), N3 (15–20%), REM (20–25%).
✅
Sleep pressure (Process S) drives deep NREM early; circadian rhythm (Process C) promotes REM toward morning.
✅
Board distinction: Early morning awakening with inability to return to sleep suggests depression — patients miss REM-rich sleep.

Neurotransmitter Regulation of Sleep-Wake States
🧠
Wake: maintained by ascending arousal systems — orexin/hypocretin (lateral hypothalamus), histamine (tuberomammillary nucleus), norepinephrine (locus coeruleus), serotonin (raphe), dopamine (VTA), acetylcholine (basal forebrain/brainstem).
🧠
NREM: promoted by GABA from ventrolateral preoptic area (VLPO) inhibiting arousal centers.
🧠
REM: driven by cholinergic REM-on neurons in pontine tegmentum; inhibited by monoaminergic REM-off neurons.
🧠
Board pearl: Narcolepsy results from loss of orexin/hypocretin neurons → inability to maintain wakefulness and intrusion of REM phenomena into wake.

Age-Related Changes in Sleep Architecture
⚡
Newborns: 16–18 hours sleep/day, 50% REM (active sleep), enter sleep through REM, polyphasic pattern.
⚡
Infants/children: REM percentage decreases to adult levels by age 5, N3 percentage highest in childhood.
⚡
Adults: consolidated monophasic pattern, 7–9 hours, standard NREM-REM cycling.
⚡
Elderly: decreased total sleep time, reduced N3 (may disappear), increased N1/N2, more fragmented sleep, earlier sleep phase.
⚡
Board pearl: Reduced slow-wave sleep in elderly contributes to memory complaints and decreased growth hormone → sarcopenia.

Sleep Deprivation and Rebound Phenomena
📌
Acute total sleep deprivation: cognitive impairment, microsleeps, mood lability, psychotic features after 48–72 hours.
📌
Chronic partial sleep deprivation: metabolic dysfunction, weight gain, insulin resistance, hypertension, immune suppression.
📌
Recovery sleep shows rebound of deprived stages: N3 rebounds first (priority for physical restoration), REM rebounds on subsequent nights.
📌
REM deprivation specifically causes irritability, difficulty concentrating, and REM rebound with intense dreams.
📌
Board pearl: Abrupt discontinuation of REM-suppressing drugs (SSRIs, TCAs) causes REM rebound with vivid dreams/nightmares.

Medications and Sleep Architecture
📣
Benzodiazepines/Z-drugs: decrease sleep latency, increase N2, suppress N3 and REM, reduce sleep quality despite increased duration.
📣
SSRIs/SNRIs: suppress REM sleep, increase REM latency, may cause insomnia or vivid dreams.
📣
TCAs: potent REM suppression, increase N3 (except clomipramine).
📣
Trazodone: increases N3, minimal REM effects — useful for depression with insomnia.
📣
Alcohol: initial sedation with REM/N3 suppression, then rebound arousals and REM in second half of night.
📣
Board pearl: Prazosin reduces nightmares in PTSD by dampening noradrenergic tone without suppressing REM.

Circadian Rhythm Integration with Sleep Architecture
🔸
Suprachiasmatic nucleus (SCN) is the master clock, entrained by light via retinohypothalamic tract.
🔸
Core body temperature nadir (~4–6 AM) coincides with maximum REM propensity and minimum alertness.
🔸
Melatonin secretion begins ~2 hours before habitual bedtime (dim light melatonin onset), promoting sleep initiation.
🔸
Cortisol nadir occurs during first half of night, rises in early morning to promote awakening.
🔸
Two-process model: homeostatic sleep drive (Process S) accumulates during wake; circadian alerting signal (Process C) opposes it until evening.
🔸
Board pearl: Delayed sleep phase disorder shows normal sleep architecture but shifted 3–6 hours later.

Polysomnography and Sleep Stage Scoring
🧷
Polysomnography simultaneously records EEG (brain waves), EOG (eye movements), EMG (muscle tone), ECG, respiratory effort, airflow, oxygen saturation.
🧷
Sleep stages scored in 30-second epochs according to predominant EEG pattern, eye movements, and muscle tone.
🧷
Sleep efficiency = total sleep time / time in bed × 100% (normal >85%).
🧷
Sleep latency = time from lights out to first epoch of sleep (normal <30 minutes).
🧷
REM latency = time from sleep onset to first REM (normal 70–100 minutes).
🧷
Board pearl: Short REM latency (<70 min) suggests narcolepsy, depression, or REM rebound.

Disorders of NREM Sleep (Parasomnias)
📍
Occur during partial arousals from N3 sleep: sleepwalking, sleep terrors, confusional arousals.
📍
Common in children (immature CNS), usually outgrown; concerning if new-onset in adults.
📍
Precipitated by sleep deprivation, fever, stress, medications that increase N3 (lithium, trazodone).
📍
Patients are difficult to arouse, have no dream recall, show complete amnesia for events.
📍
Sleep-related eating disorder: consuming food during partial arousal from NREM with amnesia.
📍
Board distinction: NREM parasomnias occur in first third of night (N3-rich); REM parasomnias in last third.

REM Sleep Behavior Disorder (RBD)
🔹
Loss of normal REM atonia allows dream enactment — patients punch, kick, yell during REM sleep.
🔹
Dreams often involve being attacked or chased, leading to injury of patient or bed partner.
🔹
Strong association with α-synucleinopathies: >80% develop Parkinson's disease, dementia with Lewy bodies, or multiple system atrophy within 10–15 years.
🔹
Polysomnography shows REM sleep without atonia (RSWA) on EMG.
🔹
Board pearl: New-onset RBD in older adults is a prodromal marker for neurodegeneration, not a primary sleep disorder.

Narcolepsy and REM Sleep Dysregulation
⭐
Type 1 narcolepsy: loss of orexin/hypocretin neurons → excessive daytime sleepiness, cataplexy, sleep paralysis, hypnagogic/hypnopompic hallucinations.
⭐
Type 2 narcolepsy: EDS without cataplexy, normal orexin levels.
⭐
Pathophysiology: inability to maintain wake states and intrusion of REM phenomena (atonia, dreams) into wakefulness.
⭐
Multiple sleep latency test (MSLT): mean sleep latency <8 minutes with ≥2 sleep-onset REM periods (SOREMPs).
⭐
Board pearl: Cataplexy (sudden bilateral loss of muscle tone triggered by emotions) is pathognomonic for type 1 narcolepsy.

Sleep Architecture in Depression
✅
Shortened REM latency (often <70 minutes, can be <45 minutes in severe cases).
✅
Increased REM density (more rapid eye movements per REM period) and increased REM percentage.
✅
Decreased N3 slow-wave sleep, impaired sleep continuity with frequent awakenings.
✅
Early morning awakening (terminal insomnia) — missing late REM-rich cycles.
✅
These changes may persist after mood symptoms resolve and predict relapse risk.
✅
Board pearl: Improved sleep architecture, particularly normalized REM latency, predicts antidepressant response.

Sleep-Disordered Breathing Effects on Architecture
🧠
Obstructive sleep apnea fragments sleep with repetitive arousals, preventing progression to deep N3 and REM sleep.
🧠
REM sleep worsens OSA due to maximum muscle atonia including upper airway dilators.
🧠
Chronic sleep fragmentation → excessive daytime sleepiness despite adequate time in bed.
🧠
CPAP therapy restores normal architecture with initial REM rebound as sleep debt repaid.
🧠
Central sleep apnea shows similar fragmentation but often with Cheyne-Stokes pattern in heart failure.
🧠
Board pearl: Supine REM sleep represents the perfect storm for OSA — maximum airway collapsibility.

Restless Legs Syndrome and Periodic Limb Movements
⚡
RLS: urge to move legs with uncomfortable sensations, worse at rest in evening, relieved by movement.
⚡
Periodic limb movements of sleep (PLMS): repetitive leg jerks every 20–40 seconds during NREM sleep.
⚡
Both fragment sleep architecture without full awakenings — patients report nonrestorative sleep.
⚡
Associated with iron deficiency (ferritin <50), pregnancy, uremia, neuropathy.
⚡
Dopamine agonists are first-line treatment; augmentation risk with long-term use.
⚡
Board pearl: RLS is a clinical diagnosis based on symptoms; PLMS requires polysomnography for diagnosis.

Chronobiology and Shift Work Effects
📌
Night shift work forces wakefulness during biological night and sleep during biological day.
📌
Results in shortened sleep duration (loss of 2–4 hours), reduced REM sleep, fragmented architecture.
📌
Chronic circadian misalignment → metabolic syndrome, cardiovascular disease, cancer risk.
📌
Rotating shifts prevent circadian adaptation, causing persistent jet lag symptoms.
📌
Melatonin, light therapy, and strategic napping can partially mitigate effects.
📌
Board pearl: Shift work sleep disorder requires both insomnia/EDS symptoms and schedule-related circadian misalignment.

Board Question Stem Patterns
📣
Child with screaming episodes in first third of night with no recall → night terrors (N3 parasomnia).
📣
Elderly man punching in sleep with dream recall → REM sleep behavior disorder, evaluate for Parkinson's.
📣
Short REM latency + sleep paralysis + daytime sleep attacks → narcolepsy type 1.
📣
Depression with 4 AM awakening unable to return to sleep → early morning awakening, REM sleep loss.
📣
Vivid nightmares after stopping paroxetine → REM rebound from SSRI withdrawal.
📣
Snoring worse in supine position during early morning → positional OSA worse in REM.
📣
College student pulls all-nighter then sleeps 14 hours → N3 rebound prioritized over REM.

One-Line Recap
🔸
Sleep architecture cycles through NREM stages (N1→N2→N3) and REM every 90–120 minutes, with early cycles dominated by restorative N3 slow-wave sleep for growth hormone release and declarative memory consolidation, while later cycles feature prolonged REM periods critical for emotional processing and procedural memory, all regulated by competing circadian (Process C) and homeostatic (Process S) drives that can be disrupted by medications, sleep disorders, and psychiatric conditions.

bottom of page