top of page

eduo
visual

Cardiovascular System
Shock classification (hypovolemic, cardiogenic, distributive, obstructive)
Core Principle of Shock
🧷
Shock is inadequate tissue perfusion to meet metabolic demands, resulting in cellular hypoxia, anaerobic metabolism, and organ dysfunction.
🧷
All forms of shock share the final common pathway of oxygen delivery (DO₂) < oxygen consumption (VO₂), leading to lactic acidosis and progressive organ failure.
🧷
The body's initial compensatory mechanisms — sympathetic activation, redistribution of blood flow, and increased oxygen extraction — can temporarily maintain blood pressure despite inadequate perfusion.
🧷
Board pearl: Shock can exist with normal blood pressure (compensated shock), making clinical signs like altered mental status, cool extremities, and elevated lactate critical early markers.

The Hemodynamic Framework
📍
Cardiac output (CO) = Heart rate × Stroke volume, where stroke volume depends on preload, contractility, and afterload.
📍
Mean arterial pressure (MAP) = CO × Systemic vascular resistance (SVR).
📍
Shock classification is based on which component fails: preload (hypovolemic), pump function (cardiogenic), vascular tone (distributive), or mechanical obstruction (obstructive).
📍
Each shock type has a characteristic hemodynamic pattern measurable by pulmonary artery catheterization: CO, SVR, and pulmonary capillary wedge pressure (PCWP).
📍
Understanding these patterns allows prediction of physical exam findings and appropriate treatment selection.

Hypovolemic Shock: Loss of Circulating Volume
🔹
Caused by hemorrhage (trauma, GI bleeding, ruptured aneurysm) or fluid loss (vomiting, diarrhea, burns, third-spacing).
🔹
Hemodynamic profile: ↓CO, ↑SVR, ↓PCWP — the body compensates for volume loss by vasoconstriction.
🔹
Clinical findings: cool extremities, weak thready pulse, flat neck veins, dry mucous membranes, decreased urine output.
🔹
Laboratory: elevated BUN:creatinine ratio (prerenal azotemia), concentrated urine (specific gravity >1.020), hemoconcentration.
🔹
Board pearl: Young healthy patients can compensate until losing 30-40% of blood volume, then suddenly decompensate — tachycardia may be the only early sign.

Stages of Hemorrhagic Shock
⭐
Class I (<15% blood volume loss): minimal symptoms, slight tachycardia, normal blood pressure.
⭐
Class II (15-30% loss): tachycardia, narrowed pulse pressure, anxiety, delayed capillary refill.
⭐
Class III (30-40% loss): hypotension, marked tachycardia, confusion, oliguria — this is when compensatory mechanisms fail.
⭐
Class IV (>40% loss): profound hypotension, obtundation, anuria, imminent cardiac arrest.
⭐
Board clue: A trauma patient with normal blood pressure but persistent tachycardia and cool extremities is in compensated (Class II) shock — immediate fluid resuscitation is indicated.

Cardiogenic Shock: Pump Failure
✅
Results from severe myocardial dysfunction: acute MI (most common), decompensated heart failure, myocarditis, arrhythmias, or valvular catastrophe.
✅
Hemodynamic profile: ↓CO, ↑SVR, ↑PCWP — the failing heart cannot generate adequate output despite elevated filling pressures.
✅
Clinical findings: cool extremities, elevated JVP, pulmonary edema (crackles), S3 gallop, hepatomegaly.
✅
Distinguishing feature: evidence of volume overload (elevated PCWP) differentiates cardiogenic from hypovolemic shock.
✅
Board pearl: Cardiogenic shock post-MI has >40% mortality and requires urgent revascularization — medical management alone is insufficient.

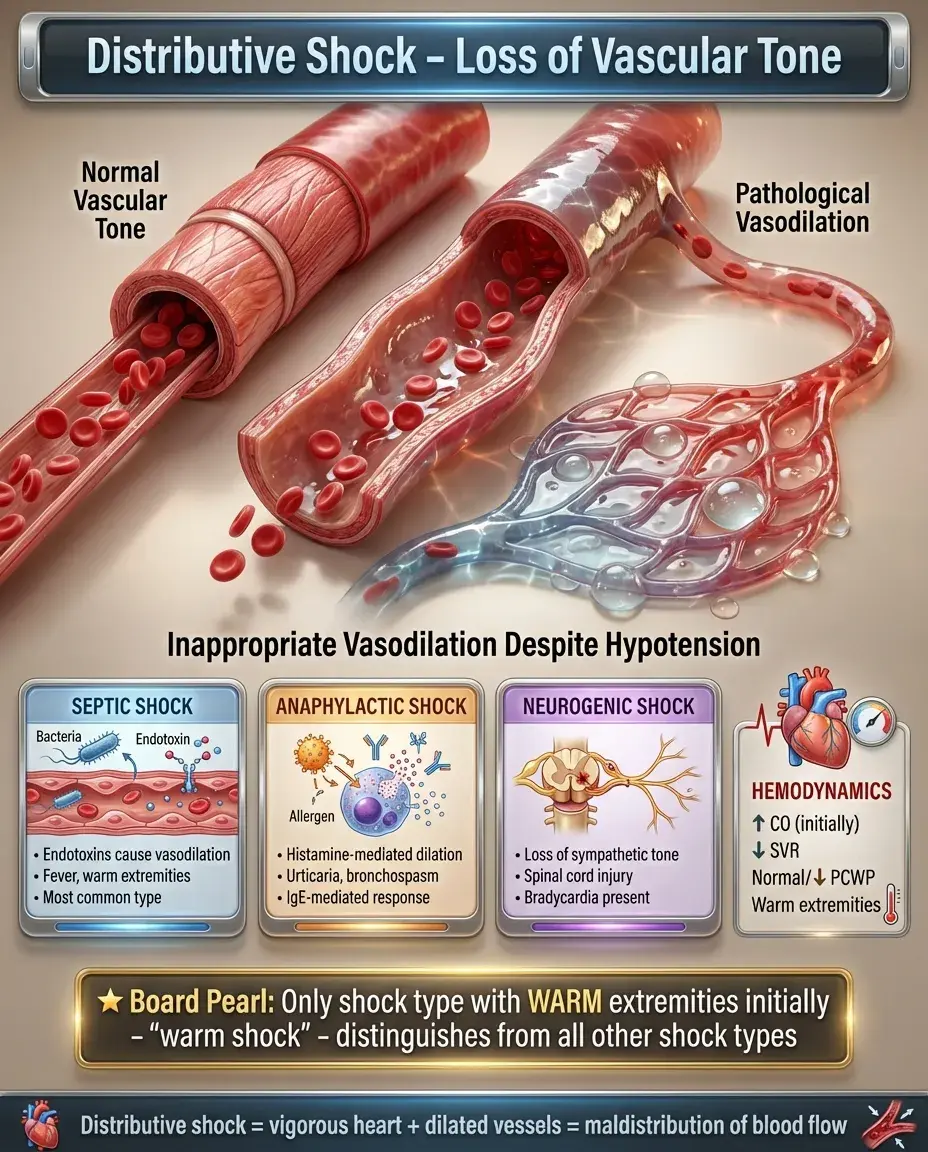
Distributive Shock: Loss of Vascular Tone
🧠
Characterized by inappropriate vasodilation despite hypotension, causing maldistribution of blood flow.
🧠
Subtypes: septic (most common), anaphylactic, neurogenic, and drug-induced.
🧠
Hemodynamic profile: ↑CO (initially), ↓SVR, normal or ↓PCWP — the heart pumps vigorously but blood pools in dilated vessels.
🧠
Clinical findings: warm extremities (early), bounding pulses, wide pulse pressure, fever (septic) or urticaria (anaphylactic).
🧠
Board distinction: Distributive shock is the only shock type with warm extremities initially — "warm shock" — though late stages show cool extremities from decompensation.
Septic Shock: The Prototypical Distributive Shock
⚡
Severe sepsis with hypotension despite adequate fluid resuscitation, requiring vasopressors to maintain MAP ≥65 mmHg.
⚡
Pathophysiology: bacterial endotoxins → cytokine storm → vasodilation, capillary leak, myocardial depression, and microvascular thrombosis.
⚡
Early (hyperdynamic) phase: ↑CO, ↓SVR, warm extremities, wide pulse pressure.
⚡
Late (hypodynamic) phase: ↓CO, cool extremities, narrow pulse pressure — resembles cardiogenic shock.
⚡
Laboratory: elevated lactate, leukocytosis or leukopenia, thrombocytopenia, coagulopathy, acute kidney injury.
⚡
Board pearl: Septic shock can present with hypothermia instead of fever, especially in elderly or immunocompromised patients.

Anaphylactic Shock: IgE-Mediated Crisis
📌
Type I hypersensitivity reaction causing massive histamine release → vasodilation, increased capillary permeability, and bronchospasm.
📌
Triggers: medications (penicillin, NSAIDs), foods (peanuts, shellfish), insect stings, latex, contrast dye.
📌
Clinical triad: cardiovascular collapse + respiratory distress (wheezing, stridor) + cutaneous findings (urticaria, angioedema).
📌
Timing: onset within minutes of exposure, though biphasic reactions can occur hours later.
📌
Laboratory: elevated tryptase levels confirm mast cell degranulation but treatment should never be delayed for testing.
📌
Board pearl: Epinephrine is the only life-saving treatment — antihistamines and steroids are adjunctive but do not reverse shock.

Neurogenic Shock: Loss of Sympathetic Tone
📣
Results from spinal cord injury above T6, disrupting sympathetic outflow while preserving parasympathetic (vagal) tone.
📣
Hemodynamic profile: ↓CO, ↓SVR, ↓HR — unique among shock types for having bradycardia instead of tachycardia.
📣
Clinical findings: hypotension with bradycardia, warm dry skin below the level of injury, priapism, loss of reflexes.
📣
Mechanism: loss of sympathetic vasoconstriction → venous pooling → decreased preload → hypotension.
📣
Board distinction: Hypotension + bradycardia + warm extremities after spinal trauma = neurogenic shock, not hypovolemic shock from internal bleeding.

Obstructive Shock: Mechanical Impediment to Flow
🔸
Physical obstruction prevents adequate cardiac output despite normal blood volume and intrinsic cardiac function.
🔸
Causes: massive PE, cardiac tamponade, tension pneumothorax, constrictive pericarditis.
🔸
Hemodynamic profile: ↓CO, ↑SVR, variable PCWP depending on which side of the heart is affected.
🔸
Common features: elevated CVP/JVP, pulsus paradoxus (tamponade), unilateral absent breath sounds (tension pneumothorax).
🔸
Board pearl: Obstructive shock often requires immediate procedural intervention — needle decompression, pericardiocentesis, or thrombolysis — rather than fluid resuscitation.

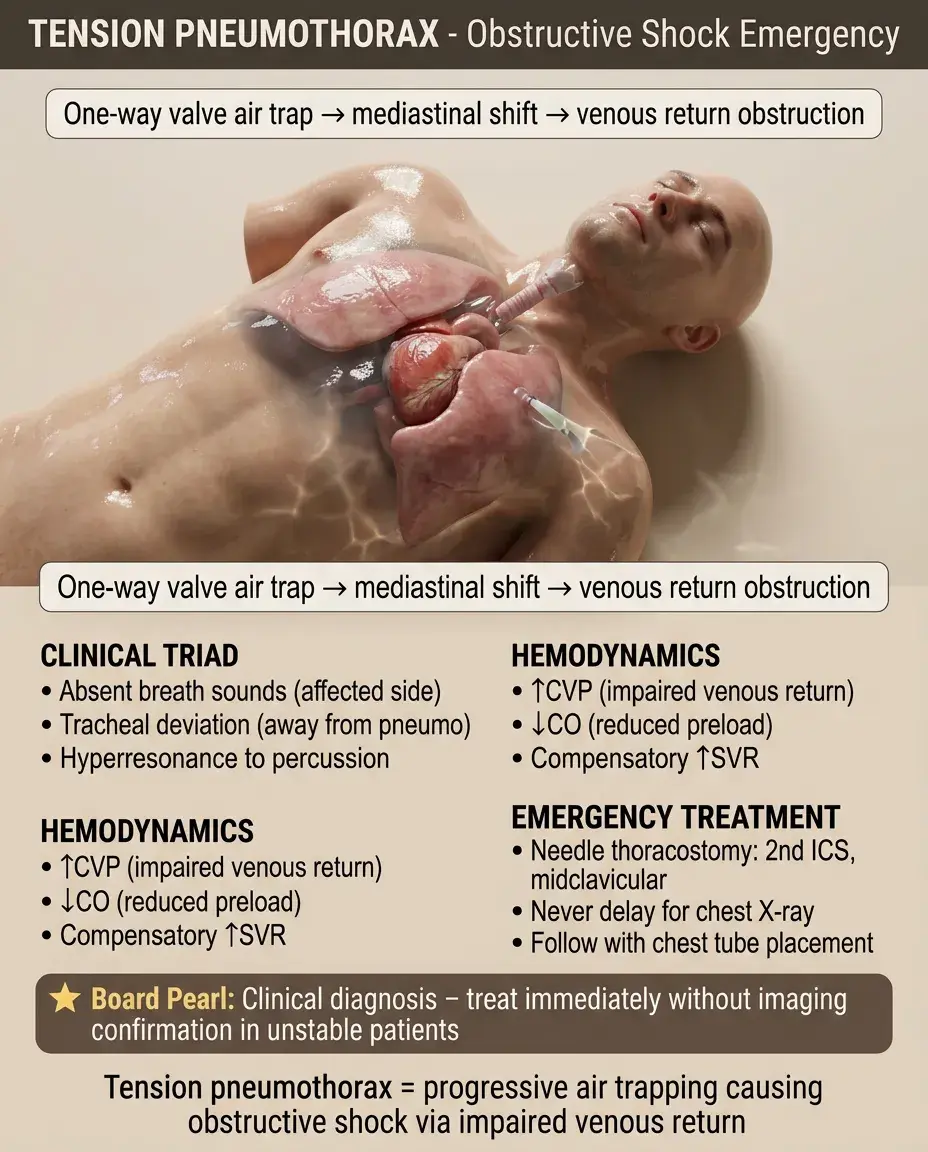
Tension Pneumothorax: The Board Favorite
🧷
Air accumulation in pleural space with one-way valve effect → progressive increase in intrapleural pressure → mediastinal shift → decreased venous return.
🧷
Clinical findings: unilateral absent breath sounds, tracheal deviation away from affected side, hyperresonance to percussion, respiratory distress.
🧷
Hemodynamics: ↑CVP from impaired venous return, ↓CO from reduced preload, compensatory ↑SVR.
🧷
Diagnosis is clinical — never delay treatment for chest X-ray confirmation in unstable patients.
🧷
Board pearl: Immediate needle thoracostomy at 2nd intercostal space, midclavicular line, followed by chest tube placement.
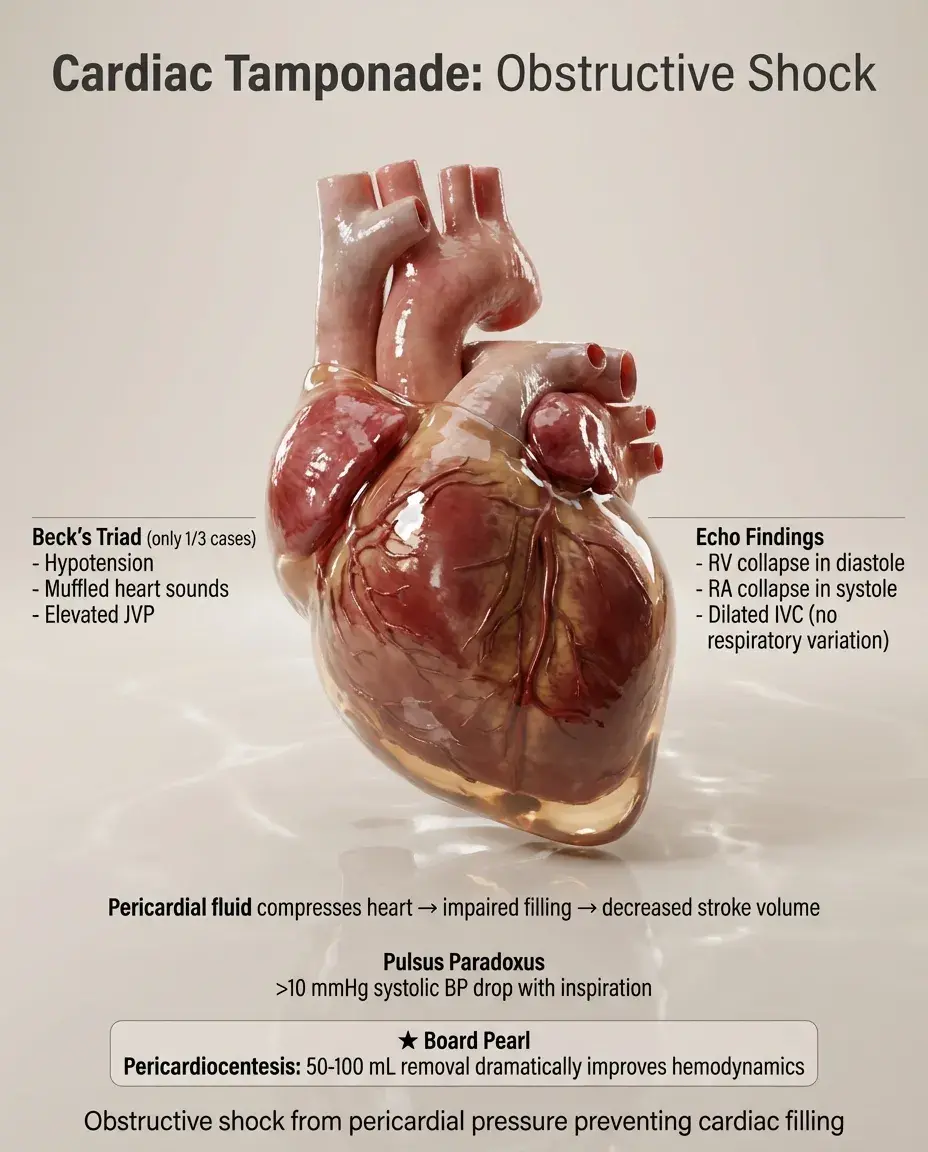
Cardiac Tamponade: Pericardial Pressure Crisis
📍
Fluid accumulation in pericardial space → increased intrapericardial pressure → impaired ventricular filling → decreased stroke volume.
📍
Beck's triad: hypotension, muffled heart sounds, elevated JVP (present in only 1/3 of cases).
📍
Pulsus paradoxus: >10 mmHg drop in systolic BP with inspiration — highly specific when present.
📍
Echo findings: RV collapse during diastole, RA collapse during systole, dilated IVC without respiratory variation.
📍
Board pearl: Pericardiocentesis is both diagnostic and therapeutic — removal of even 50-100 mL can dramatically improve hemodynamics.
Mixed and Sequential Shock States
🔹
Real patients often have multiple shock mechanisms operating simultaneously or evolving over time.
🔹
Septic shock frequently combines distributive (vasodilation) with hypovolemic (capillary leak) and cardiogenic (septic cardiomyopathy) components.
🔹
Hemorrhagic shock can trigger inflammatory cascades leading to distributive physiology.
🔹
Prolonged shock of any type → myocardial dysfunction → cardiogenic component ("shocked heart").
🔹
Board approach: Identify the predominant mechanism first, then recognize and treat additional components as they develop.

Compensatory Mechanisms Across Shock Types
⭐
Sympathetic activation: ↑heart rate, ↑contractility, vasoconstriction → maintains blood pressure initially.
⭐
Renin-angiotensin-aldosterone activation: sodium/water retention, vasoconstriction.
⭐
ADH release: water retention, vasoconstriction.
⭐
Redistribution of blood flow: away from skin, GI tract, kidneys → toward brain and heart.
⭐
Increased oxygen extraction: tissues extract more O₂ from each RBC, widening the arteriovenous O₂ difference.
⭐
Board pearl: Cool extremities in shock reflect successful compensation (vasoconstriction), except in early distributive shock where vasodilation dominates.

Laboratory Markers of Shock Severity
✅
Lactate: elevated in all shock types due to anaerobic metabolism — level correlates with mortality, clearance predicts survival.
✅
Base deficit: negative base excess reflects metabolic acidosis from tissue hypoperfusion.
✅
ScvO₂ (central venous oxygen saturation): <70% indicates increased oxygen extraction due to inadequate delivery.
✅
Acute kidney injury: elevated creatinine, oliguria — reflects renal hypoperfusion.
✅
Liver dysfunction: elevated transaminases, coagulopathy — "shock liver" from hepatic hypoperfusion.
✅
Board pearl: Lactate >4 mmol/L defines shock severity regardless of blood pressure — it's tissue perfusion, not pressure, that matters.

The Microcirculation in Shock
🧠
Shock ultimately damages the microcirculation: capillary endothelial dysfunction, microthrombi formation, and impaired oxygen delivery.
🧠
Septic shock shows the most severe microcirculatory dysfunction: heterogeneous flow with some capillaries hyperperfused while adjacent ones have no flow.
🧠
Prolonged vasoconstriction in other shock types → microcirculatory "no-reflow" phenomenon even after macrocirculatory parameters normalize.
🧠
This explains why early aggressive treatment improves outcomes — preventing irreversible microcirculatory damage.
🧠
Clinical correlate: Persistent lactate elevation despite normalized blood pressure indicates ongoing microcirculatory dysfunction.

Pitfalls in Shock Recognition
⚡
Young patients compensate remarkably well — normal blood pressure doesn't exclude shock.
⚡
Beta-blockers and calcium channel blockers blunt tachycardia — absence of tachycardia doesn't exclude shock.
⚡
Elderly patients have baseline hypertension — "normal" blood pressure may represent relative hypotension.
⚡
Early septic shock can present with normal or elevated blood pressure due to high cardiac output.
⚡
Spinal shock (neurologic dysfunction after spinal injury) differs from neurogenic shock (hemodynamic instability from sympathetic loss).
⚡
Board pearl: Always calculate shock index (HR/SBP) — values >0.9 suggest occult shock even with normal vital signs.

Treatment Principles by Shock Type
📌
Hypovolemic: aggressive fluid resuscitation (crystalloid or blood products), control source of loss.
📌
Cardiogenic: cautious fluids if truly volume depleted, inotropes, treat underlying cause (revascularization for MI).
📌
Distributive: aggressive fluids first, then vasopressors (norepinephrine first-line), source control for sepsis, epinephrine for anaphylaxis.
📌
Obstructive: immediate relief of obstruction — needle decompression, pericardiocentesis, thrombolysis for massive PE.
📌
All types: ensure adequate oxygenation, monitor lactate clearance, prevent complications.
📌
Board pearl: Fluid challenge helps differentiate shock types — improvement suggests hypovolemic, worsening suggests cardiogenic.

Board Question Stem Patterns
📣
Trauma patient with tachycardia and cool extremities but normal BP → Class II hemorrhagic shock.
📣
Post-MI patient with pulmonary edema and cool extremities → cardiogenic shock.
📣
Fever + hypotension + warm extremities initially → septic shock.
📣
Spinal injury + hypotension + bradycardia + warm extremities → neurogenic shock.
📣
Chest trauma + absent breath sounds + tracheal deviation → tension pneumothorax.
📣
Muffled heart sounds + JVD + hypotension → cardiac tamponade.
📣
Hypotension that improves with leg raise → hypovolemic or distributive; worsens with leg raise → cardiogenic.
📣
Shock + elevated lactate but normal blood pressure → compensated shock, aggressive treatment indicated.

One-Line Recap
🔸
Shock classification follows hemodynamic patterns — hypovolemic (↓preload, ↓CO, ↑SVR), cardiogenic (↓pump function, ↓CO, ↑SVR, ↑PCWP), distributive (↓vascular tone, ↑CO initially, ↓SVR), and obstructive (mechanical barrier, ↓CO, ↑SVR) — each with distinct clinical findings that guide immediate life-saving interventions while lactate tracks tissue perfusion regardless of blood pressure.

bottom of page