top of page

eduo
visual

Respiratory System
Pleural effusion (transudate vs exudate, Light’s criteria)
Core Principle of Pleural Effusions
🧷
Pleural effusions represent abnormal fluid accumulation in the pleural space between the visceral and parietal pleura.
🧷
The fundamental distinction is between transudates (caused by systemic factors altering hydrostatic or oncotic pressure) and exudates (caused by local pleural inflammation increasing capillary permeability).
🧷
This distinction drives both the diagnostic workup and treatment approach — transudates require treating the underlying systemic condition while exudates often need targeted pleural intervention.
🧷
Light's criteria provide the definitive method for differentiating these two categories based on protein and LDH measurements.

Pathophysiology of Transudate Formation
📍
Transudates result from imbalances in Starling forces: increased hydrostatic pressure (CHF, fluid overload) or decreased oncotic pressure (hypoalbuminemia from cirrhosis, nephrotic syndrome).
📍
The pleural capillaries remain intact — fluid leaks passively due to pressure gradients, not inflammation.
📍
Because the barrier function is preserved, large molecules like proteins and LDH remain in the vascular space, resulting in low concentrations in the pleural fluid.
📍
Board pearl: Transudates are "ultrafiltrates" of plasma — think of them as watery leaks through an intact but overwhelmed barrier.

Pathophysiology of Exudate Formation
🔹
Exudates result from increased capillary permeability due to pleural inflammation, infection, or malignancy.
🔹
Inflammatory mediators disrupt endothelial junctions, allowing proteins, cells, and enzymes to escape into the pleural space.
🔹
Common causes include pneumonia (parapneumonic effusion), malignancy, pulmonary embolism, rheumatoid arthritis, and tuberculosis.
🔹
The damaged pleural surface also produces LDH locally, further elevating pleural fluid levels.
🔹
Board pearl: Exudates are "inflammatory leaks" — the barrier is damaged, not just overwhelmed.

Light's Criteria: The Gold Standard
⭐
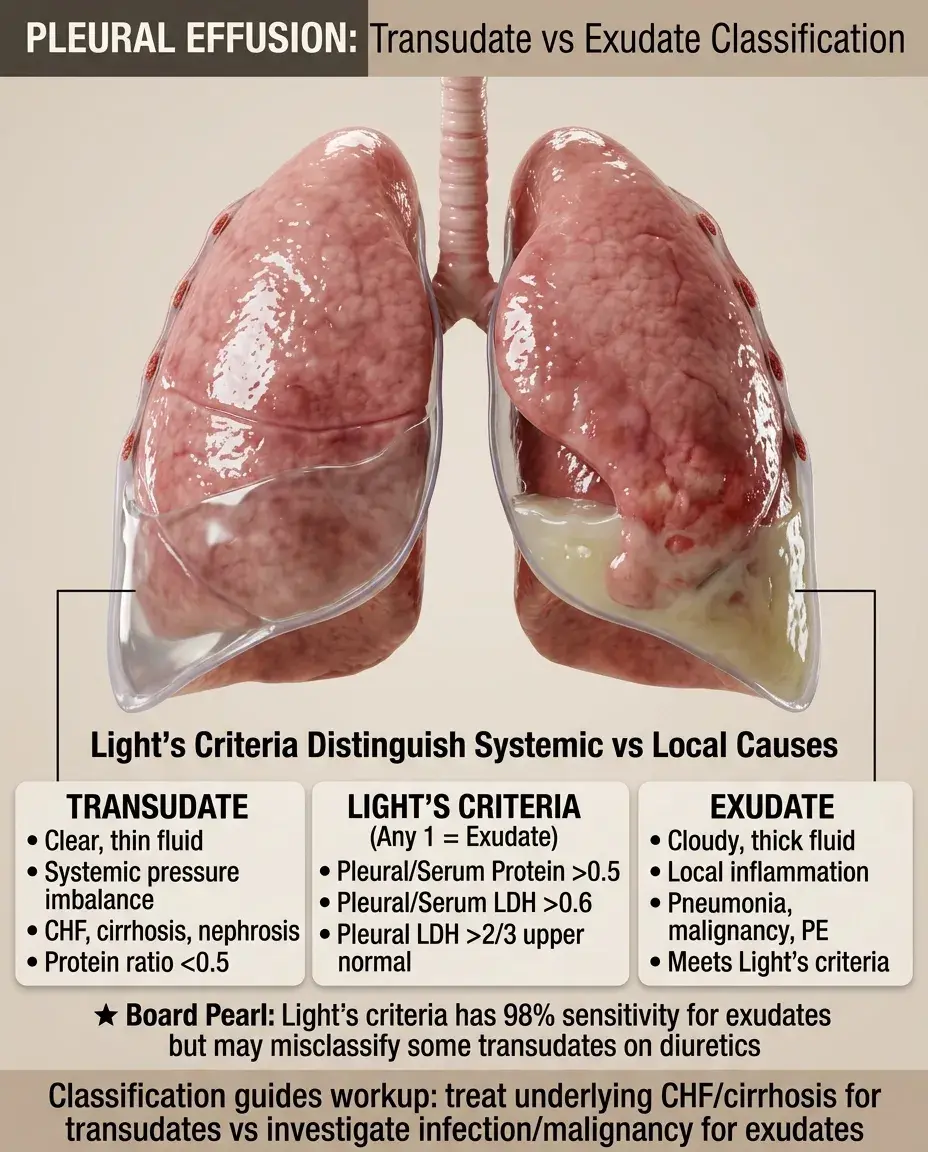
An effusion is exudative if ANY ONE of the following is met:
⭐
Pleural fluid protein/serum protein ratio > 0.5
⭐
Pleural fluid LDH/serum LDH ratio > 0.6
⭐
Pleural fluid LDH > 2/3 the upper limit of normal for serum LDH
⭐
Sensitivity for exudates approaches 98% but specificity is only 80% — some transudates (especially after diuresis) can be misclassified.
⭐
Board pearl: If even one criterion is positive, classify as exudate. All three must be negative to call it transudate.

Clinical Application of Light's Criteria
✅
Always obtain simultaneous pleural fluid and serum samples — the ratios require both values.
✅
Calculate all three criteria even if one is already positive — this provides redundancy and confirms the classification.
✅
In borderline cases where clinical suspicion strongly suggests transudate but Light's criteria indicate exudate, consider the serum-pleural albumin gradient.
✅
If serum albumin − pleural albumin > 1.2 g/dL, the effusion is likely a transudate despite meeting Light's criteria.
✅
Board clue: Questions often provide all the numbers needed to calculate Light's criteria — do the math.

Common Transudative Causes
🧠
Congestive heart failure (most common overall cause of pleural effusion) — usually bilateral, right > left if unilateral.
🧠
Cirrhosis with hepatic hydrothorax — usually right-sided due to diaphragmatic defects.
🧠
Nephrotic syndrome — bilateral effusions with severe hypoalbuminemia.
🧠
Atelectasis — small effusions from reduced pleural pressure.
🧠
Peritoneal dialysis — fluid crossing through diaphragmatic pores.
🧠
Board pearl: Bilateral effusions in a patient with JVD, S3 gallop, and peripheral edema → CHF until proven otherwise.

Common Exudative Causes
⚡
Parapneumonic effusion/empyema — most common exudative cause, associated with bacterial pneumonia.
⚡
Malignancy — lung cancer, breast cancer, lymphoma, mesothelioma; often bloody.
⚡
Pulmonary embolism — occurs in 30-50% of PE cases, usually small and unilateral.
⚡
Tuberculosis — lymphocyte-predominant, high adenosine deaminase (ADA).
⚡
Rheumatoid arthritis — very low glucose (<30 mg/dL), low pH, cholesterol crystals.
⚡
Board pearl: Unilateral effusion in a smoker with weight loss → malignancy until proven otherwise.

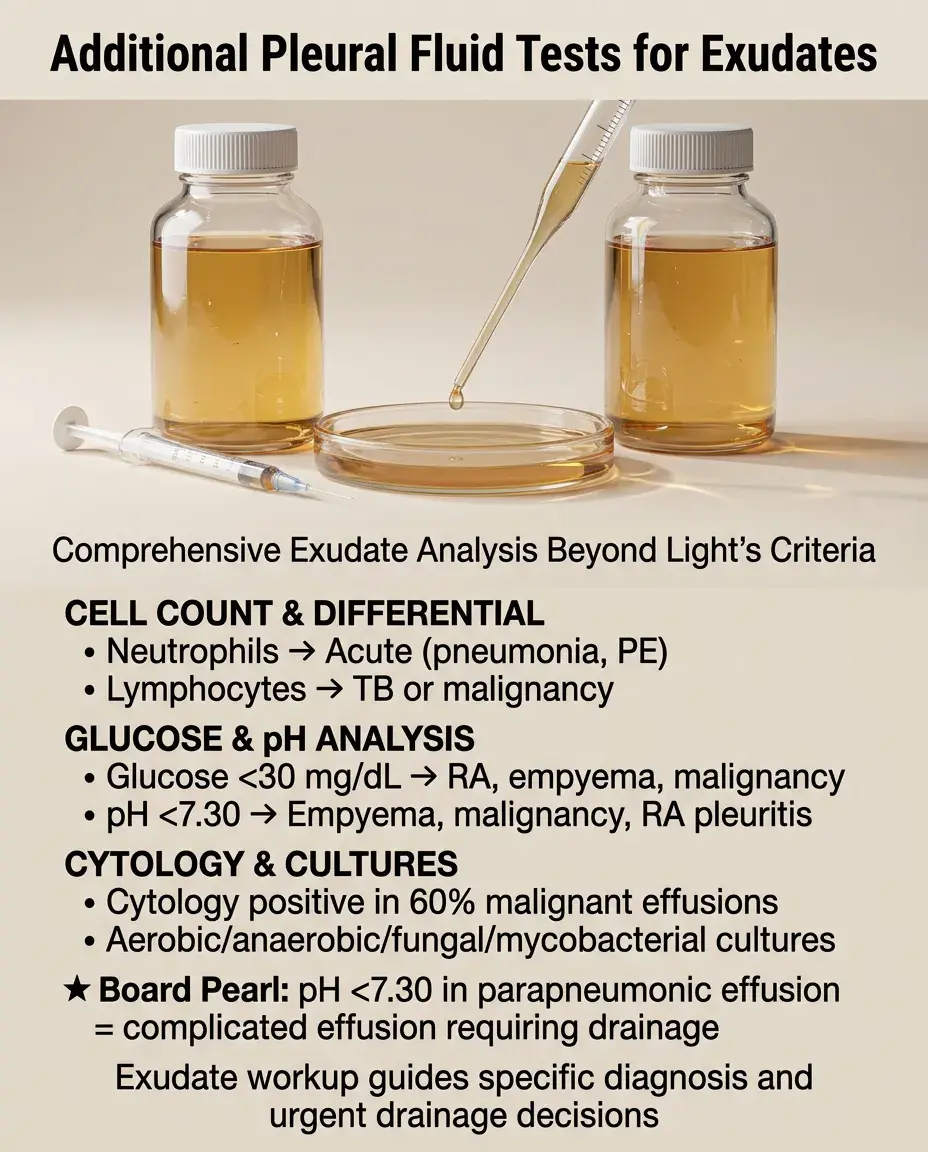
Additional Pleural Fluid Tests for Exudates
📌
Cell count and differential — neutrophil predominance suggests acute process (pneumonia, PE); lymphocyte predominance suggests TB or malignancy.
📌
Glucose — very low (<30 mg/dL) in rheumatoid arthritis, empyema, malignant effusion.
📌
pH — <7.30 indicates empyema, malignancy, or rheumatoid pleuritis; requires tube thoracostomy if parapneumonic.
📌
Cytology — positive in 60% of malignant effusions on first tap.
📌
Cultures — aerobic, anaerobic, fungal, mycobacterial as indicated.
📌
Board pearl: pH <7.30 in parapneumonic effusion = complicated effusion requiring drainage.
Parapneumonic Effusions and Empyema Progression
📣
Simple parapneumonic: sterile exudate, pH >7.30, glucose >60 mg/dL, LDH <1000 IU/L → antibiotics alone.
📣
Complicated parapneumonic: pH <7.30, glucose <60 mg/dL, LDH >1000 IU/L, positive Gram stain/culture → requires drainage.
📣
Empyema: frank pus in pleural space, positive culture, septations on ultrasound → requires drainage, may need surgery.
📣
Board distinction: The transition from simple → complicated → empyema represents increasing need for invasive management beyond antibiotics.

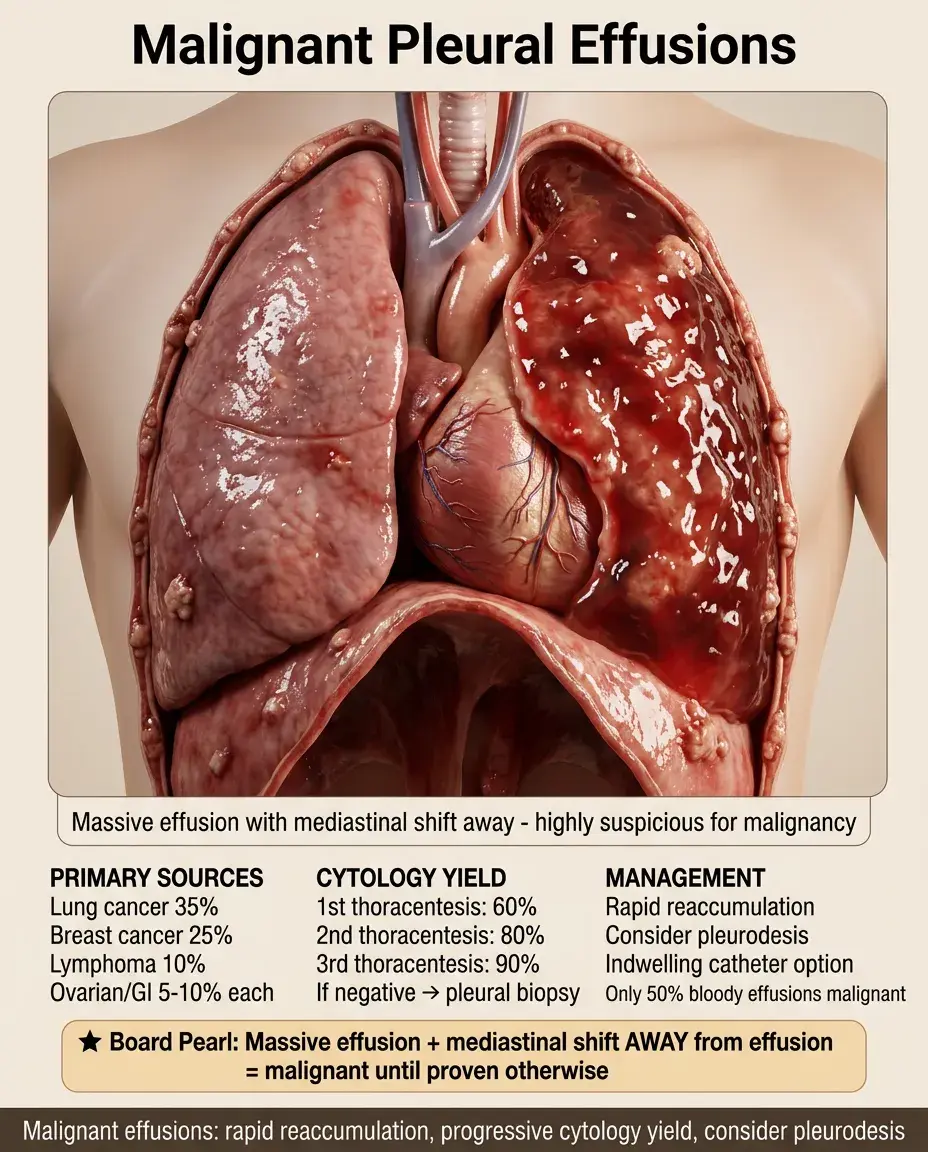
Malignant Pleural Effusions
🔸
Most common primary tumors: lung (35%), breast (25%), lymphoma (10%), ovarian/GI (5-10% each).
🔸
Often bloody but only 50% of bloody effusions are malignant — also consider PE, trauma.
🔸
Cytology sensitivity: 60% on first thoracentesis, 80% with second, 90% with third.
🔸
If cytology negative but suspicion high → pleural biopsy or thoracoscopy.
🔸
Malignant effusions reaccumulate rapidly — consider pleurodesis or indwelling catheter.
🔸
Board pearl: Massive effusion with mediastinal shift away from the effusion → malignant until proven otherwise.
Chylothorax and Pseudochylothorax
🧷
Chylothorax: true chyle leak from thoracic duct injury — trauma, surgery, malignancy (lymphoma).
🧷
Milky appearance, triglycerides >110 mg/dL, presence of chylomicrons on lipoprotein electrophoresis.
🧷
Pseudochylothorax: cholesterol accumulation from chronic inflammation — rheumatoid arthritis, TB.
🧷
Also milky but triglycerides <50 mg/dL, cholesterol >200 mg/dL, cholesterol crystals on microscopy.
🧷
Board distinction: High triglycerides = chylothorax (acute); high cholesterol = pseudochylothorax (chronic).

Hemothorax Recognition and Management
📍
Defined as pleural fluid hematocrit >50% of peripheral blood hematocrit.
📍
Causes: trauma (most common), malignancy, PE, aortic rupture, coagulopathy.
📍
Unlike bloody pleural effusion, hemothorax doesn't clot due to defibrination by pleural motion.
📍
Requires urgent drainage to prevent fibrothorax and trapped lung.
📍
Board pearl: Pleural fluid that looks like blood → check pleural hematocrit. If >50% of serum → hemothorax requiring chest tube.

Hepatic Hydrothorax Mechanisms
🔹
Occurs in 5-10% of cirrhotic patients, usually with ascites but can occur in isolation.
🔹
Mechanism: ascitic fluid crosses diaphragm through microscopic defects, usually on right side.
🔹
Negative intrathoracic pressure during inspiration pulls fluid from peritoneum to pleura.
🔹
Confirmed by injecting technetium-99m sulfur colloid into peritoneum and detecting in pleural space.
🔹
Board pearl: Right-sided transudate in a cirrhotic patient even without clinically apparent ascites → hepatic hydrothorax.

Pleural Fluid in Pulmonary Embolism
⭐
Present in 30-50% of PE cases, usually small and unilateral.
⭐
Can be either transudate (from atelectasis) or exudate (from lung infarction).
⭐
Often bloody if lung infarction has occurred.
⭐
Pleural fluid findings are nonspecific — diagnosis requires imaging (CTA or V/Q scan).
⭐
Board clue: Small unilateral effusion + pleuritic chest pain + risk factors for DVT → think PE, not just pneumonia.

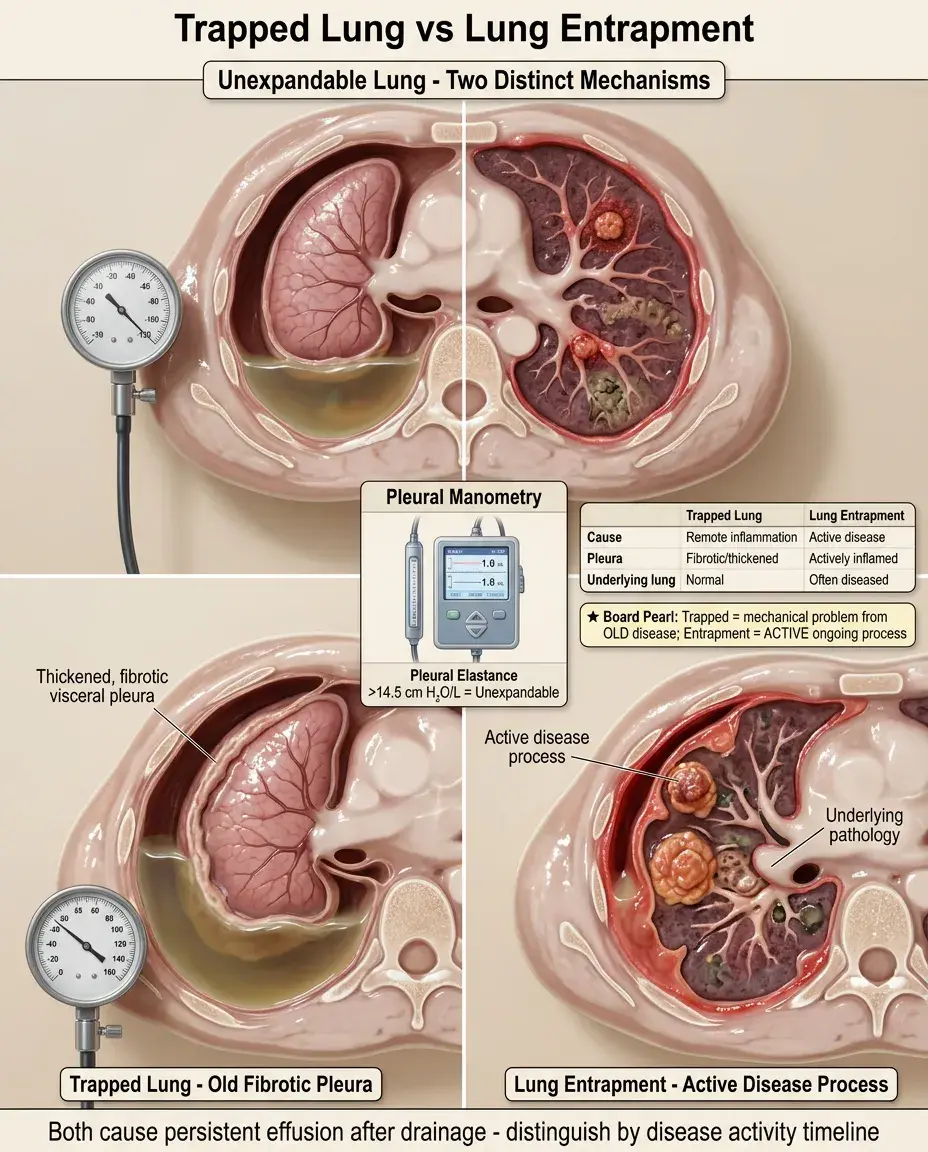
Trapped Lung vs Lung Entrapment
✅
Trapped lung: visceral pleura thickened by remote inflammation prevents lung expansion; pleural pressure becomes very negative with fluid removal.
✅
Lung entrapment: active pleural inflammation/malignancy prevents expansion; underlying lung may also be diseased.
✅
Both cause persistent effusion after drainage and "unexpandable lung" on chest X-ray.
✅
Pleural manometry showing elastance >14.5 cm H₂O/L suggests unexpandable lung.
✅
Board distinction: Trapped lung is a mechanical problem from old disease; entrapment involves active disease.
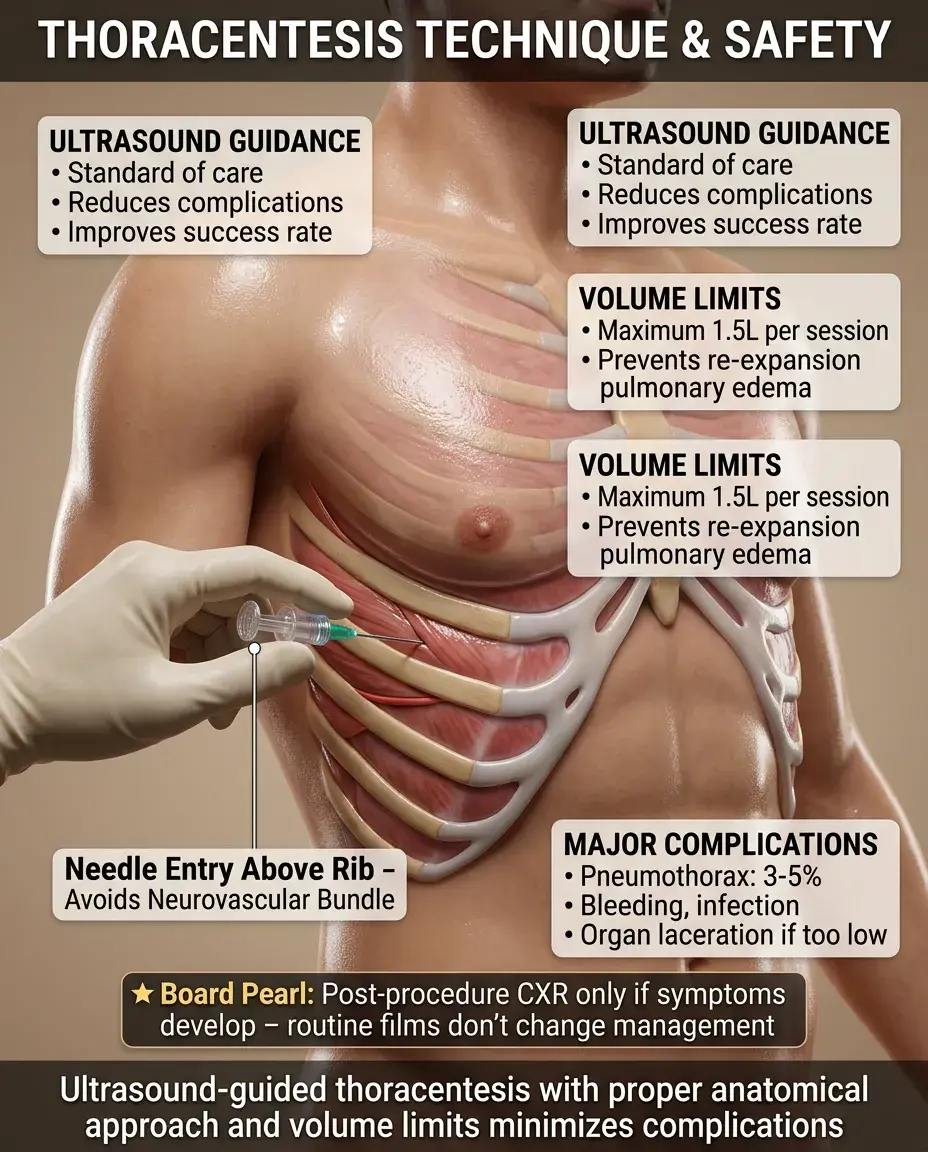
Thoracentesis Technique and Complications
🧠
Ultrasound guidance reduces complications and improves success rate — now standard of care.
🧠
Patient sits upright, leaning forward; needle enters above rib to avoid neurovascular bundle.
🧠
Remove no more than 1.5 L at once to avoid re-expansion pulmonary edema.
🧠
Complications: pneumothorax (3-5%), bleeding, infection, splenic/hepatic laceration if too low.
🧠
Board pearl: Post-procedure chest X-ray is indicated only if symptoms develop — routine films don't change management.
Special Considerations in Bilateral Effusions
⚡
Bilateral transudates: think CHF first, then hypoalbuminemia states (cirrhosis, nephrotic syndrome).
⚡
Bilateral exudates are rare: consider malignancy, rheumatologic disease, or drugs (amiodarone, methotrexate).
⚡
If bilateral but asymmetric, tap the larger side — if exudate, must tap both sides as causes may differ.
⚡
Board approach: Bilateral effusions + cardiomegaly + B-lines on lung ultrasound → CHF, treat without thoracentesis unless atypical features.

Integration with Other Diagnostic Modalities
📌
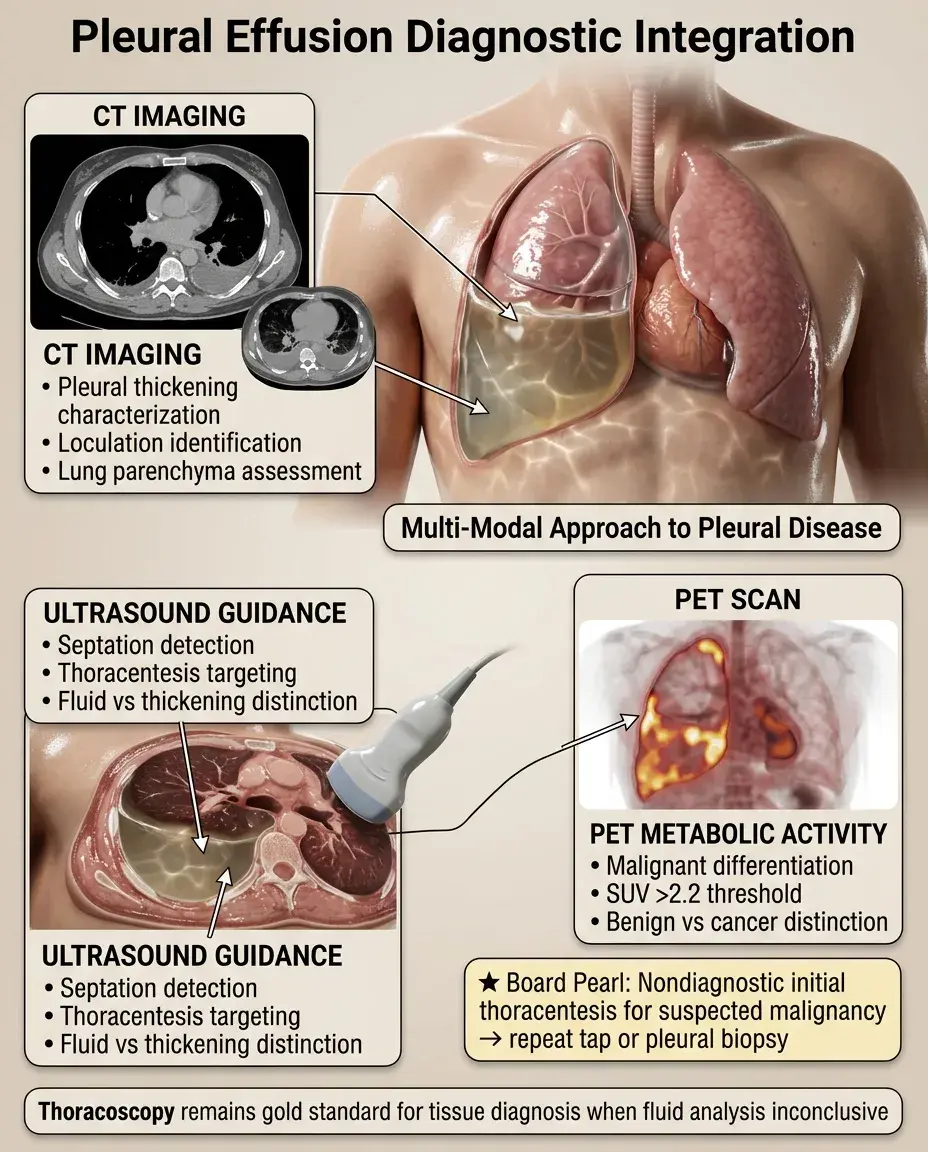
Chest CT: better characterizes pleural thickening, loculations, underlying lung parenchyma.
📌
Ultrasound: identifies septations, guides thoracentesis, distinguishes fluid from pleural thickening.
📌
PET scan: helps differentiate malignant from benign pleural thickening (SUV >2.2 suggests malignancy).
📌
Thoracoscopy: gold standard for pleural biopsy when diagnosis remains unclear after thoracentesis.
📌
Board pearl: If initial thoracentesis is nondiagnostic for suspected malignancy → repeat thoracentesis or proceed to pleural biopsy.
Board Question Stem Patterns
📣
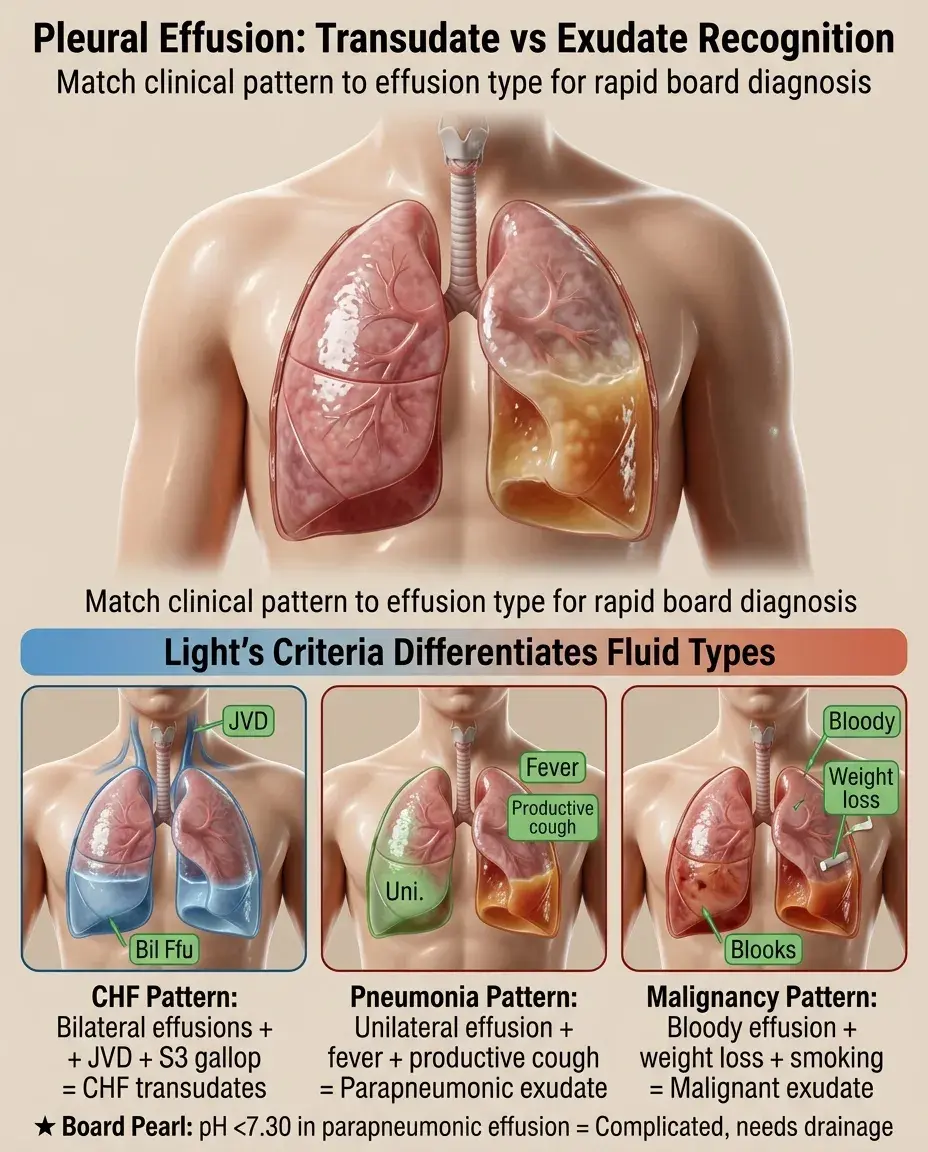
Bilateral effusions + JVD + S3 gallop → CHF-related transudates.
📣
Unilateral effusion + fever + productive cough → parapneumonic effusion, check pH and glucose.
📣
Bloody effusion + weight loss + smoking history → malignancy, send cytology.
📣
Milky effusion after cardiac surgery → chylothorax from thoracic duct injury.
📣
Right effusion + ascites + spider angiomata → hepatic hydrothorax.
📣
Effusion + pleuritic pain + Wells criteria → PE, order CTA.
📣
pH <7.30 in parapneumonic effusion → complicated effusion requiring drainage.
One-Line Recap
🔸
Pleural effusions are classified as transudates (systemic pressure/oncotic imbalances) or exudates (local inflammation/malignancy) using Light's criteria — pleural/serum protein >0.5, pleural/serum LDH >0.6, or pleural LDH >2/3 upper normal limit — guiding further workup toward treating underlying CHF/cirrhosis for transudates versus investigating for pneumonia/malignancy/PE in exudates.
bottom of page