top of page

eduo
visual

Biostatistics & Epidemiology
Pandemic Response and Surveillance Systems
Core Principle of Pandemic Response and Surveillance Systems
🧷
Pandemic response requires coordinated detection, tracking, and intervention across local, national, and global health systems to identify emerging threats before widespread transmission occurs.
🧷
Surveillance systems serve as the early warning mechanism — continuously monitoring disease patterns, detecting aberrations from baseline, and triggering public health responses.
🧷
The fundamental challenge is balancing sensitivity (catching all outbreaks) with specificity (avoiding false alarms) while maintaining rapid response capability.
🧷
Board questions test understanding of surveillance types, outbreak investigation steps, and the hierarchy of pandemic response measures from least to most restrictive.

Types of Disease Surveillance Systems
📍
Passive surveillance: healthcare providers report notifiable diseases to health departments — inexpensive but underestimates true incidence due to underreporting.
📍
Active surveillance: public health officials proactively contact providers to seek cases — more complete but resource-intensive.
📍
Sentinel surveillance: selected sites or providers report all cases of specific conditions — provides high-quality data from representative locations.
📍
Syndromic surveillance: monitors symptoms (fever, cough, diarrhea) before diagnosis — enables early outbreak detection.
📍
Board pearl: Passive surveillance is the backbone of routine disease monitoring; active surveillance is reserved for high-priority conditions or outbreak investigations.

Notifiable Disease Reporting Requirements
🔹
Nationally notifiable diseases must be reported to CDC through state health departments — includes conditions like tuberculosis, measles, hepatitis, STIs, and emerging infections.
🔹
Reporting timelines vary: immediately reportable (anthrax, plague, smallpox), within 24 hours (measles, meningococcal disease), or within one week (HIV, tuberculosis).
🔹
Healthcare providers and laboratories both have independent reporting obligations — dual reporting increases capture completeness.
🔹
Board distinction: Individual patient consent is NOT required for notifiable disease reporting — public health authority supersedes privacy concerns for communicable diseases.
🔹
Failure to report is both an ethical violation and often illegal under state public health laws.

Outbreak Detection and Epidemic Curves
⭐
An outbreak is an increase in cases above the expected baseline for a given population, place, and time — requires knowing the endemic level.
⭐
Epidemic curves plot cases over time, revealing transmission patterns: point source (single peak), continuous source (plateau), propagated (multiple waves).
⭐
The shape of the epidemic curve combined with the incubation period helps identify the likely exposure source and transmission mode.
⭐
Board clue: A sharp peak followed by gradual decline suggests point source exposure; successive peaks separated by one incubation period indicate person-to-person spread.
⭐
Early outbreak detection depends on astute clinicians recognizing unusual disease patterns and reporting promptly.

Steps in Outbreak Investigation
✅
1) Verify the outbreak — confirm diagnoses and determine if cases exceed expected baseline.
✅
2) Define and identify cases — establish case definition based on clinical criteria, time, place, and person characteristics.
✅
3) Collect data — demographics, exposures, timeline of illness using standardized questionnaires.
✅
4) Generate hypotheses — analyze data for common exposures or risk factors.
✅
5) Test hypotheses — use analytical epidemiology (case-control or cohort studies).
✅
6) Implement control measures — may begin before investigation complete if source suspected.
✅
7) Communicate findings — to healthcare providers, public, and policymakers.
✅
Board pearl: Control measures often start during hypothesis generation, not after confirmation.

Contact Tracing Principles
🧠
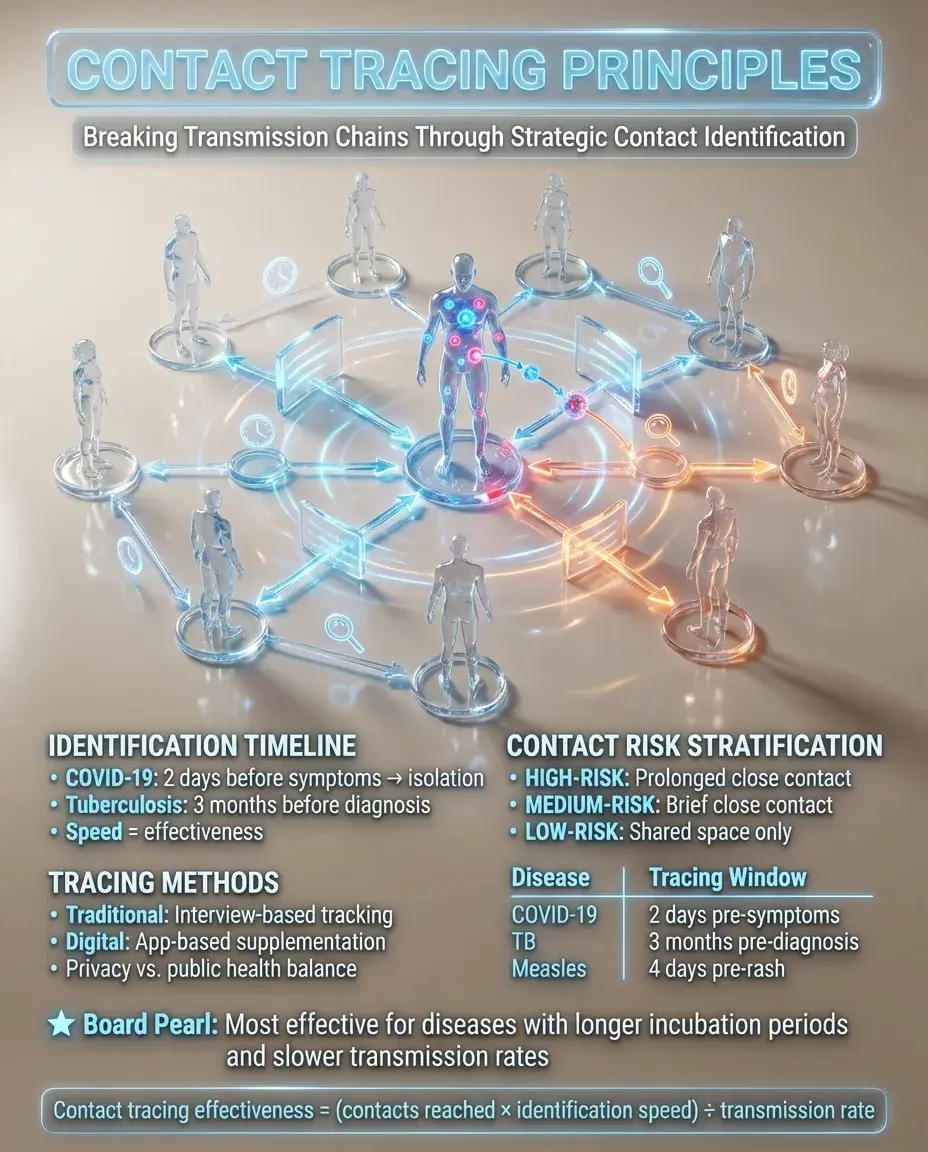
Contact tracing identifies and monitors individuals exposed to infectious cases to break transmission chains — effectiveness depends on the proportion of contacts reached and speed of identification.
🧠
The infectious period determines when to trace: for COVID-19, 2 days before symptom onset through isolation period; for tuberculosis, 3 months before diagnosis.
🧠
Contacts are stratified by exposure risk: high-risk (prolonged close contact), medium-risk (brief close contact), low-risk (shared space without close contact).
🧠
Digital contact tracing supplements traditional methods but raises privacy concerns — balancing public health benefit with individual privacy rights.
🧠
Board pearl: Contact tracing is most effective for diseases with longer incubation periods and slower transmission rates.
Isolation vs Quarantine — Critical Distinctions
⚡
Isolation separates sick individuals with communicable diseases from healthy people — applies to confirmed or suspected cases.
⚡
Quarantine restricts movement of well individuals who were exposed but are not yet ill — prevents transmission during incubation period.
⚡
Duration depends on disease: isolation until no longer infectious, quarantine for maximum incubation period.
⚡
Board distinction: Isolation is for sick people; quarantine is for exposed but well people.
⚡
Legal authority exists for mandatory isolation/quarantine, but voluntary compliance is preferred — coercion is a last resort.
⚡
Modern quarantine often allows home confinement rather than designated facilities.

Non-Pharmaceutical Interventions (NPIs)
📌
NPIs are public health measures that reduce transmission without vaccines or medications — crucial early in pandemics before medical countermeasures available.
📌
Individual level: hand hygiene, respiratory etiquette, mask-wearing, physical distancing.
📌
Community level: school closures, mass gathering cancellations, business restrictions, stay-at-home orders.
📌
Effectiveness depends on community compliance, timing of implementation, and disease transmission characteristics.
📌
Board concept: NPIs are most effective when layered (multiple interventions simultaneously) and implemented early in community transmission.
📌
The goal is to 'flatten the curve' — reduce peak healthcare demand even if total cases remain similar.

International Health Regulations and Global Coordination
📣
The International Health Regulations (IHR) are legally binding rules requiring countries to report public health emergencies of international concern (PHEICs) to WHO.
📣
Core capacities required: surveillance, reporting, verification, response, and risk communication at points of entry.
📣
WHO declares PHEICs based on: seriousness, unusual/unexpected nature, international spread risk, and travel/trade restriction risk.
📣
Board pearl: Countries must report potential PHEICs within 24 hours of assessment — includes novel influenza, SARS, MERS, polio, and other emerging threats.
📣
Global surveillance networks like GOARN (Global Outbreak Alert and Response Network) coordinate international response.

Laboratory Networks and Diagnostic Capacity
🔸
The Laboratory Response Network (LRN) provides tiered diagnostic capacity: sentinel labs (initial screening), reference labs (confirmation), national labs (specialized testing).
🔸
During pandemics, rapid diagnostic development and deployment is critical — balancing speed with accuracy validation.
🔸
Diagnostic capacity must scale from hundreds to millions of tests — requires supply chain management, personnel training, and quality assurance.
🔸
Board concept: Initial outbreak investigation often relies on syndromic diagnosis while awaiting laboratory confirmation — clinical case definitions guide early response.
🔸
Genomic surveillance tracks viral evolution, variant emergence, and transmission chains.

Risk Communication During Health Emergencies
🧷
Effective risk communication follows principles of transparency, timeliness, empathy, and acknowledgment of uncertainty.
🧷
Messages must be clear, consistent across agencies, and actionable — avoiding technical jargon while maintaining accuracy.
🧷
Trust is the foundation — built through honest acknowledgment of what is known, unknown, and being done to learn more.
🧷
Board principle: Communicate early and often, even with incomplete information — silence creates information voids filled by misinformation.
🧷
Cultural competence and addressing health literacy barriers ensures equitable information access.
🧷
Social media monitoring helps identify and counter misinformation rapidly.

Vaccine Development and Distribution in Pandemics
📍
Traditional vaccine development takes 10-15 years; pandemic timelines compress to 12-18 months through parallel processing and platform technologies.
📍
Priority groups for limited vaccine supply: healthcare workers, essential workers, high-risk populations (elderly, chronic conditions), then general population.
📍
Distribution challenges include cold chain requirements, multi-dose regimens, and reaching underserved populations.
📍
Board concept: Allocation frameworks balance multiple ethical principles — maximizing benefit, minimizing harm, promoting justice, and reciprocity for those accepting occupational risk.
📍
Vaccine effectiveness monitoring continues post-deployment through adverse event surveillance and breakthrough infection tracking.

Healthcare System Surge Capacity
🔹
Surge capacity is the ability to manage sudden influxes of patients — requires expanding staff, stuff (supplies), space, and systems.
🔹
Crisis standards of care shift from individual-focused to population-focused decisions when resources are overwhelmed.
🔹
Triage protocols prioritize patients most likely to benefit — may exclude those too well or too sick to benefit from scarce resources.
🔹
Board distinction: Conventional capacity uses usual resources; contingency adapts practices but maintains similar outcomes; crisis involves difficult resource allocation decisions.
🔹
Surge planning includes canceling elective procedures, expanding ICU capacity, and training non-critical care staff.

Supply Chain Management and Strategic National Stockpile
⭐
The Strategic National Stockpile maintains medical supplies for public health emergencies — includes PPE, ventilators, medications, and vaccines.
⭐
Just-in-time supply chains are efficient but vulnerable to disruption — pandemics require shift to resilience over efficiency.
⭐
Critical supplies during respiratory pandemics: N95 respirators, ventilators, sedatives, paralytics, and eventually vaccines and therapeutics.
⭐
Board concept: Supply allocation follows ethical frameworks similar to vaccines — prioritizing healthcare workers, high-risk patients, and essential services.
⭐
International supply chain disruption necessitates domestic manufacturing capacity for critical items.

Behavioral and Social Factors in Pandemic Response
✅
Individual behavior change is essential for NPI effectiveness — influenced by risk perception, self-efficacy, social norms, and trust in authorities.
✅
Pandemic fatigue leads to decreasing compliance over time — requires renewed messaging and support for sustainable behaviors.
✅
Social determinants create differential pandemic impact: crowded housing, essential work, limited healthcare access compound risk for vulnerable populations.
✅
Board pearl: Behavioral interventions must address barriers — providing masks/sanitizer, paid sick leave, isolation support — not just information.
✅
Community engagement and trusted messengers are crucial for reaching populations with historical mistrust of government.

Data Systems and Real-Time Analytics
🧠
Effective pandemic response requires integrated data systems linking clinical, laboratory, and epidemiologic information in real-time.
🧠
Key metrics include: case counts, test positivity rates, hospitalization rates, ICU capacity, mortality, and vaccination coverage.
🧠
Data visualization through dashboards enables rapid situation awareness for decision-makers and public transparency.
🧠
Board concept: Leading indicators (cases, test positivity) predict lagging indicators (hospitalizations, deaths) by 2-4 weeks — enabling proactive response.
🧠
Privacy-preserving record linkage allows tracking outcomes while protecting individual identity.
🧠
Modeling projections guide resource allocation but require constant updating with real-world data.

Legal and Ethical Framework for Pandemic Response
⚡
Public health police powers derive from states' authority to protect population health — includes isolation, quarantine, and business restrictions.
⚡
Ethical principles in tension: individual autonomy vs collective benefit, liberty vs security, privacy vs surveillance needs.
⚡
Due process protections apply even in emergencies — restrictions must be necessary, proportionate, and least restrictive to achieve public health goals.
⚡
Board distinction: Federal government coordinates and supports but cannot directly order state public health measures — federalism shapes pandemic response.
⚡
International human rights law permits derogations during emergencies but core rights remain non-derogable.

Recovery and Building Resilient Health Systems
📌
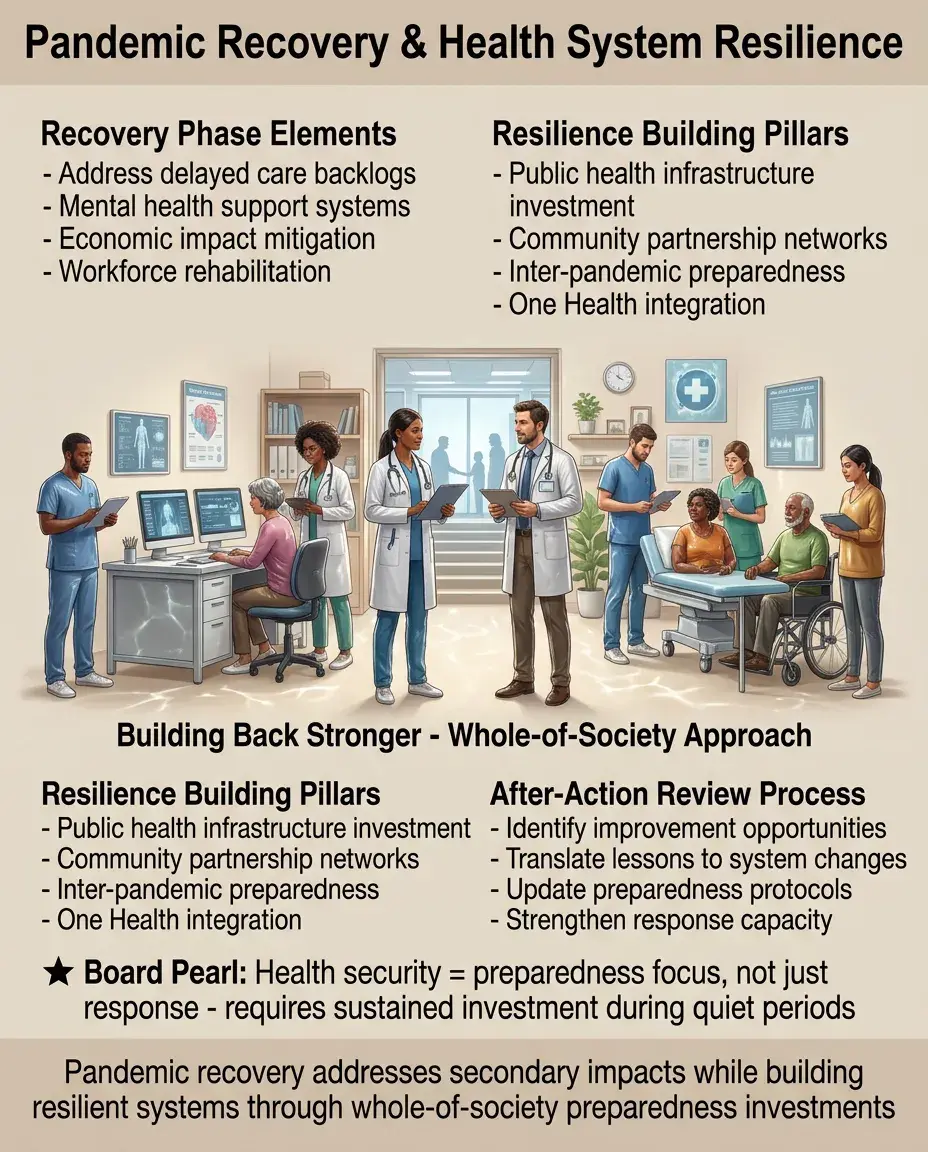
Pandemic recovery involves not just controlling transmission but addressing secondary health impacts: delayed care, mental health, economic consequences.
📌
Building resilience requires sustained investment in public health infrastructure, workforce, and community partnerships during inter-pandemic periods.
📌
After-action reviews identify improvement opportunities — must translate lessons learned into concrete system changes.
📌
Board concept: Health security is achieved through preparedness, not just response — requires whole-of-society approach beyond health sector.
📌
One Health approach recognizes interconnections between human, animal, and environmental health in preventing future pandemics.
Board Question Stem Patterns
📣
Healthcare worker exposed to patient later diagnosed with measles → immediate post-exposure prophylaxis with MMR vaccine if not immune.
📣
Unusual cluster of pneumonia cases in previously healthy adults → activate outbreak investigation protocol, report to health department.
📣
Limited vaccine supply during pandemic → prioritize healthcare workers and high-risk populations using ethical allocation framework.
📣
Restaurant-associated gastroenteritis outbreak with sharp epidemic curve peak → point source outbreak, likely contaminated food.
📣
Patient refuses isolation for active tuberculosis → last resort involuntary isolation with due process protections.
📣
Novel respiratory virus spreading internationally → WHO assessment for PHEIC declaration under IHR.

One-Line Recap
🔸
Pandemic response integrates surveillance systems for early detection, outbreak investigation to identify sources, non-pharmaceutical interventions and vaccines to reduce transmission, surge capacity to manage healthcare demand, risk communication to guide behavior, and global coordination under International Health Regulations — all balanced against ethical principles and individual rights while addressing disparate impacts on vulnerable populations.

bottom of page