top of page

eduo
visual

Behavioral Health & Nervous System
Mechanisms of Psychotropic Medications
Core Principle of Psychotropic Medications
🧷
Psychotropic medications alter neurotransmitter signaling to treat psychiatric conditions. Their mechanisms, side effects, and drug interactions are predictable from their receptor and transporter pharmacology.
🧷
Board questions focus on mechanism of action, major side effects, dangerous interactions, and matching the drug class to the clinical indication.
🧷
The major categories are antidepressants, antipsychotics, mood stabilizers, anxiolytics, and stimulants.

SSRIs: Mechanism and Clinical Use
📍
Selective serotonin reuptake inhibitors block SERT, increasing serotonin in the synaptic cleft.
📍
First-line treatment for major depressive disorder, GAD, panic disorder, social anxiety, OCD, PTSD, and bulimia.
📍
Onset of therapeutic effect requires 4–6 weeks (time needed for receptor downregulation and neural adaptation).
📍
Common side effects: GI disturbance (nausea, diarrhea), sexual dysfunction (delayed orgasm, decreased libido), weight gain, insomnia or sedation.
📍
Board pearl: SSRIs are first-line for nearly all anxiety and depressive disorders. Sexual dysfunction is the most common reason for discontinuation.

SSRIs: Dangerous Interactions and Serotonin Syndrome
🔹
Serotonin syndrome: excess serotonergic activity producing a triad of neuromuscular excitability (clonus, hyperreflexia, tremor), autonomic instability (hyperthermia, tachycardia, diaphoresis), and altered mental status (agitation, confusion).
🔹
Most commonly caused by combining two serotonergic agents: SSRIs + MAOIs is the most dangerous combination. Also SSRIs + tramadol, meperidine, linezolid, triptans, or St. John’s wort.
🔹
Treatment: discontinue the offending agent(s), supportive care, cyproheptadine (5-HT2A antagonist) for severe cases.
🔹
Board pearl: Serotonin syndrome = clonus + hyperthermia + agitation. Distinguish from neuroleptic malignant syndrome (NMS) which has lead-pipe RIGIDITY (not clonus) and is caused by dopamine blockade.

SNRIs and Atypical Antidepressants
⭐
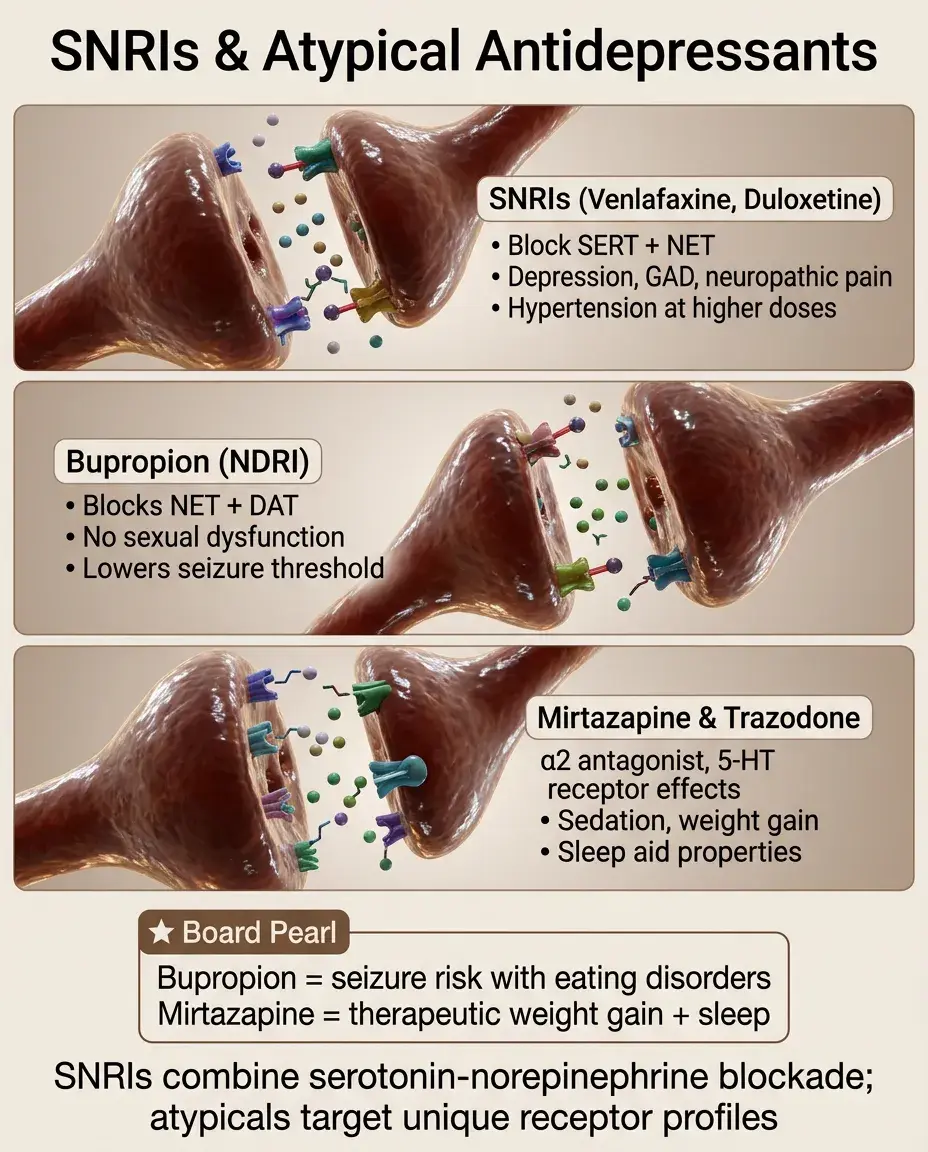
SNRIs (venlafaxine, duloxetine): block both SERT and NET. Used for depression, GAD, neuropathic pain (duloxetine), and fibromyalgia. Side effects similar to SSRIs plus hypertension (from NE reuptake blockade) at higher doses.
⭐
Bupropion: blocks NET and DAT (norepinephrine-dopamine reuptake inhibitor). Used for depression, smoking cessation, and as an adjunct to avoid SSRI-induced sexual dysfunction. Lowers seizure threshold — contraindicated in eating disorders and seizure disorders.
⭐
Mirtazapine: alpha-2 antagonist (increases NE and 5-HT release) + 5-HT2 and 5-HT3 antagonist + H1 antagonist. Causes sedation and weight gain. Useful for depressed patients with insomnia and poor appetite.
⭐
Trazodone: 5-HT2A antagonist and weak SERT inhibitor. Primarily used as a sleep aid at low doses. Risk of priapism.
⭐
Board pearl: Bupropion = no sexual dysfunction, no weight gain, lowers seizure threshold. Mirtazapine = sedation + weight gain (can be therapeutic).
Tricyclic Antidepressants (TCAs)
✅
Block SERT and NET (like SNRIs) but ALSO block muscarinic (M1), histamine (H1), and alpha-1 adrenergic receptors.
✅
Examples: amitriptyline, nortriptyline, imipramine, clomipramine (strongest serotonergic TCA, used for OCD).
✅
Side effects from receptor blockade: anticholinergic (dry mouth, constipation, urinary retention, blurred vision, tachycardia), sedation (H1), orthostatic hypotension (alpha-1).
✅
TCA overdose is life-threatening: cardiac toxicity from Na⁺ channel blockade producing QRS widening, arrhythmias, seizures, and death. Treat with sodium bicarbonate.
✅
Board pearl: TCA overdose = widened QRS + seizures + anticholinergic toxicity. Treatment = sodium bicarbonate (overcomes Na⁺ channel block). TCAs are the most lethal antidepressants in overdose.

MAOIs
🧠
Irreversibly inhibit monoamine oxidase, preventing degradation of serotonin, norepinephrine, and dopamine.
🧠
Used for treatment-resistant and atypical depression.
🧠
Two critical interactions: tyramine-containing foods → hypertensive crisis. Serotonergic drugs → serotonin syndrome.
🧠
Must wait 2 weeks after stopping an MAOI before starting an SSRI (and vice versa for fluoxetine, which has a long half-life).
🧠
Board pearl: MAOIs are the most dangerous antidepressants regarding drug and food interactions. The 2-week washout period is critical.

First-Generation (Typical) Antipsychotics
⚡
Mechanism: D2 receptor blockade in the mesolimbic pathway → reduces positive symptoms of psychosis (hallucinations, delusions).
⚡
High-potency (haloperidol, fluphenazine): strong D2 blockade → more extrapyramidal symptoms (EPS), less sedation/anticholinergic effects.
⚡
Low-potency (chlorpromazine, thioridazine): weaker D2 blockade but stronger muscarinic, histaminic, and alpha-1 blockade → more sedation, anticholinergic effects, orthostatic hypotension, but fewer EPS.
⚡
Board pearl: High-potency typicals = more EPS, less sedation. Low-potency typicals = more sedation/anticholinergic, less EPS.

Extrapyramidal Symptoms (EPS)
📌
Acute dystonia: sustained involuntary muscle contractions (torticollis, oculogyric crisis) within hours to days of starting an antipsychotic. Treat with benztropine (anticholinergic) or diphenhydramine.
📌
Akathisia: subjective restlessness and inability to sit still. Days to weeks after starting. Treat with beta-blockers or benzodiazepines.
📌
Bradykinesia/parkinsonism: rigidity, tremor, shuffling gait. Weeks to months. Treat with benztropine or amantadine.
📌
Tardive dyskinesia: involuntary choreiform movements of the face, tongue, and limbs. Months to years of use. Often irreversible. Treat with valbenazine or deutetrabenazine (VMAT2 inhibitors).
📌
Board pearl: EPS timeline: hours (dystonia) → days (akathisia) → weeks (parkinsonism) → months-years (tardive dyskinesia).

Neuroleptic Malignant Syndrome (NMS)
📣
A life-threatening reaction to dopamine antagonists (antipsychotics, metoclopramide) or abrupt withdrawal of dopaminergic drugs (levodopa).
📣
Features: lead-pipe muscle rigidity, hyperthermia, altered mental status, and autonomic instability (tachycardia, labile BP, diaphoresis). Elevated creatine kinase (CK) from rhabdomyolysis.
📣
Treatment: discontinue the offending agent, dantrolene (muscle relaxant), bromocriptine (dopamine agonist), supportive care.
📣
Board pearl: NMS = rigidity + hyperthermia + elevated CK + dopamine blockade. Distinguish from serotonin syndrome (clonus, not rigidity, serotonergic drugs). NMS develops over days; serotonin syndrome develops within hours.

Second-Generation (Atypical) Antipsychotics
🔸
Mechanism: D2 blockade PLUS 5-HT2A blockade. The serotonin antagonism is thought to reduce EPS risk and may improve negative symptoms and cognition.
🔸
Examples: risperidone, olanzapine, quetiapine, aripiprazole, clozapine, ziprasidone, lurasidone.
🔸
Major metabolic side effects: weight gain, hyperglycemia, dyslipidemia, metabolic syndrome. Olanzapine and clozapine carry the highest metabolic risk.
🔸
Board pearl: Atypicals have fewer EPS than typicals but cause more metabolic syndrome. Olanzapine and clozapine = highest weight gain and metabolic risk.

Clozapine
🧷
The most effective antipsychotic for treatment-resistant schizophrenia (defined as failure of ≥2 adequate antipsychotic trials).
🧷
Unique and dangerous side effect: agranulocytosis (potentially fatal drop in neutrophils) in approximately 1–2% of patients. Requires mandatory regular absolute neutrophil count (ANC) monitoring.
🧷
Other side effects: seizures (dose-dependent), severe metabolic syndrome, sedation, sialorrhea (paradoxical drooling despite anticholinergic properties), myocarditis.
🧷
Board pearl: Clozapine = treatment-resistant schizophrenia + mandatory ANC monitoring for agranulocytosis. It is the only antipsychotic proven effective for refractory cases.

Lithium
📍
The gold-standard mood stabilizer for bipolar disorder. Effective for acute mania, maintenance therapy, and has unique anti-suicidal properties.
📍
Narrow therapeutic index: therapeutic range 0.6–1.2 mEq/L. Toxicity produces tremor, ataxia, confusion, seizures, and renal failure.
📍
Side effects: nephrogenic diabetes insipidus (lithium blocks ADH action at V2 receptors → polyuria, polydipsia), hypothyroidism, tremor, weight gain, teratogenicity (Ebstein anomaly — downward displacement of the tricuspid valve).
📍
Board pearl: Lithium toxicity is precipitated by dehydration, NSAIDs, ACE inhibitors, and thiazide diuretics (all reduce lithium clearance). Ebstein anomaly = lithium in pregnancy.

Valproic Acid and Carbamazepine
🔹
Valproic acid: mood stabilizer and antiepileptic. Mechanism involves increased GABA (inhibits GABA transaminase), Na⁺ channel blockade, and T-type Ca²⁺ channel blockade. Side effects: hepatotoxicity, pancreatitis, thrombocytopenia, weight gain, teratogenicity (neural tube defects — spina bifida).
🔹
Carbamazepine: mood stabilizer and antiepileptic. Mechanism: Na⁺ channel blockade. Side effects: aplastic anemia, agranulocytosis, SIADH, Stevens-Johnson syndrome (associated with HLA-B*1502 in East Asian populations), teratogenicity (neural tube defects). Also a potent CYP450 inducer (autoinduction).
🔹
Board pearl: Valproic acid = neural tube defects + hepatotoxicity. Carbamazepine = neural tube defects + aplastic anemia + SJS + CYP450 induction.

Lamotrigine
⭐
Mood stabilizer primarily effective for bipolar depression (less effective for acute mania). Also used as an antiepileptic.
⭐
Mechanism: Na⁺ channel blockade and glutamate release inhibition.
⭐
Must be titrated slowly to avoid Stevens-Johnson syndrome (SJS) / toxic epidermal necrolysis (TEN), a potentially fatal mucocutaneous reaction. Risk increased by rapid dose escalation and concomitant valproate (which inhibits lamotrigine metabolism).
⭐
Board pearl: Lamotrigine = bipolar depression + must titrate slowly to prevent SJS. Valproate raises lamotrigine levels — use half the usual dose when combining.

Benzodiazepines
✅
Mechanism: enhance GABA-A receptor function by increasing the frequency of Cl⁻ channel opening (require GABA to be present — they are allosteric modulators, not direct agonists).
✅
Uses: acute anxiety, panic attacks, insomnia, seizures (status epilepticus), alcohol withdrawal, procedural sedation.
✅
Side effects: sedation, respiratory depression, anterograde amnesia, dependence, tolerance.
✅
Withdrawal: potentially life-threatening — seizures, delirium, autonomic instability. Must taper gradually.
✅
Flumazenil: competitive benzodiazepine antagonist at the GABA-A receptor. Use with caution — can precipitate seizures in chronic users.
✅
Board pearl: Benzodiazepine withdrawal can be fatal (seizures). Barbiturate overdose is more dangerous than benzodiazepine overdose because barbiturates directly open Cl⁻ channels independent of GABA.

Stimulants
🧠
Methylphenidate: blocks DAT and NET, increasing synaptic dopamine and norepinephrine. First-line for ADHD.
🧠
Amphetamines (mixed amphetamine salts, lisdexamfetamine): block DAT/NET AND cause reverse transport (active release) of dopamine and norepinephrine from vesicles. Also first-line for ADHD.
🧠
Side effects: insomnia, decreased appetite, weight loss, tachycardia, hypertension. Risk of growth suppression in children. Potential for abuse.
🧠
Board pearl: Methylphenidate = reuptake blockade only. Amphetamines = reuptake blockade + active monoamine release. Both increase dopamine and NE in the prefrontal cortex to improve attention.

Medications for Substance Use Disorders
⚡
Alcohol: naltrexone (mu opioid antagonist, reduces craving and reward), acamprosate (modulates glutamate/GABA balance), disulfiram (inhibits aldehyde dehydrogenase → acetaldehyde accumulates → nausea/flushing with alcohol, aversion therapy).
⚡
Opioids: methadone (long-acting mu agonist, maintenance), buprenorphine (partial mu agonist, has a ceiling effect on respiratory depression), naltrexone (mu antagonist, relapse prevention).
⚡
Nicotine: varenicline (partial nicotinic receptor agonist, reduces craving and reward), bupropion (NET/DAT blocker), nicotine replacement.
⚡
Board pearl: Disulfiram + alcohol = acetaldehyde accumulation (nausea, flushing, headache). Naltrexone is used for both alcohol and opioid use disorders.

Clinical Pitfalls
📌
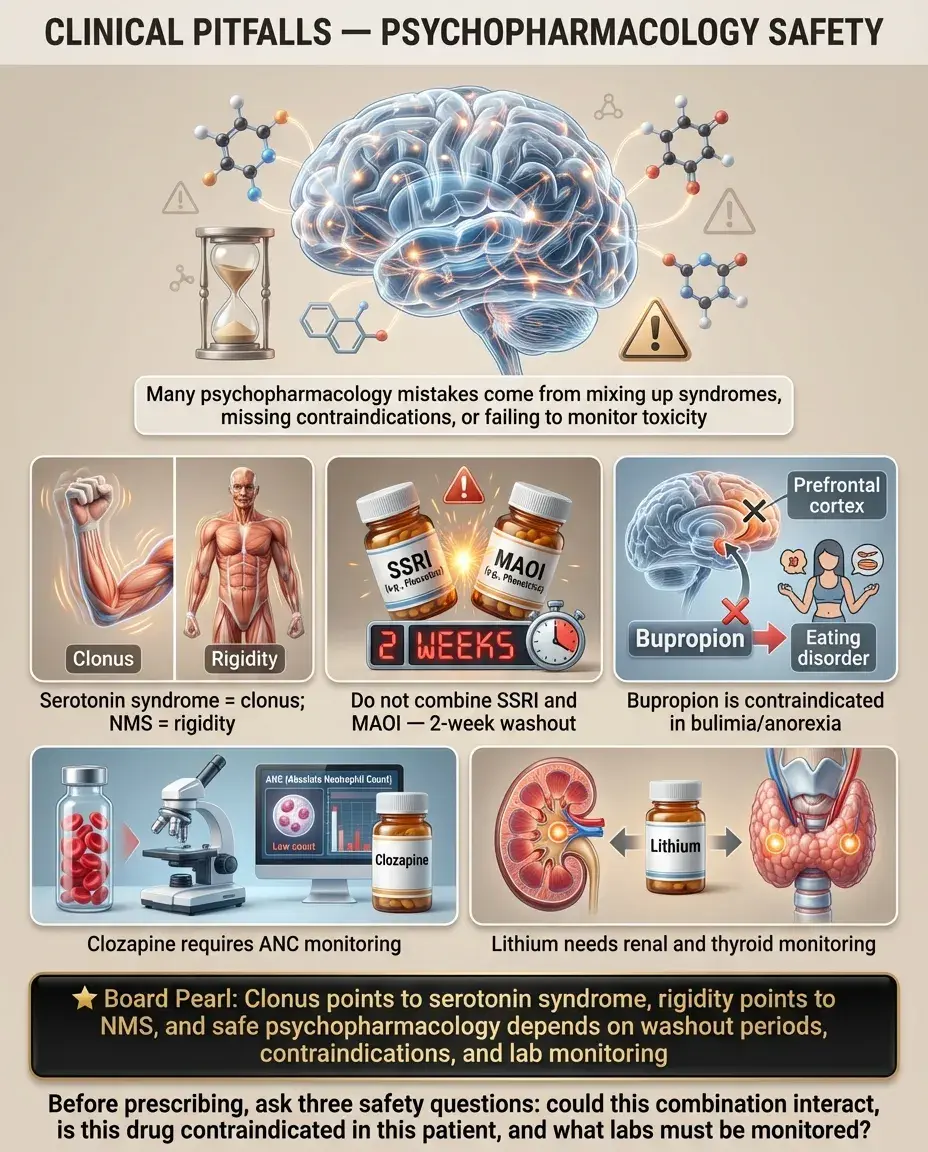
Confusing serotonin syndrome and NMS: serotonin syndrome = clonus + hyperthermia + serotonergic drug. NMS = rigidity + hyperthermia + dopamine antagonist.
📌
Starting an SSRI and MAOI simultaneously or without a washout period: 2-week gap required.
📌
Prescribing bupropion to a patient with an eating disorder: lowers seizure threshold, contraindicated in bulimia/anorexia.
📌
Forgetting that clozapine requires ANC monitoring: agranulocytosis is the critical risk.
📌
Using lithium without monitoring renal and thyroid function: causes nephrogenic DI and hypothyroidism.
Board Question Stem Patterns
📣
Patient on SSRI and tramadol develops clonus, hyperthermia, agitation → serotonin syndrome.
📣
Patient on haloperidol develops lead-pipe rigidity, fever, elevated CK → NMS.
📣
Patient on antipsychotic for 2 years develops involuntary lip smacking and tongue movements → tardive dyskinesia.
📣
Patient on lithium develops polyuria and dilute urine unresponsive to desmopressin → nephrogenic DI.
📣
Pregnant patient on valproate — what is the teratogenic risk? → neural tube defects.
📣
Treatment-resistant schizophrenia patient needs the most effective antipsychotic → clozapine (with ANC monitoring).
📣
Patient develops rash while rapidly titrating lamotrigine → SJS risk, must titrate slowly.
📣
Widened QRS on ECG after intentional overdose of amitriptyline → TCA toxicity, treat with sodium bicarbonate.

One-Line Recap
🔸
Psychotropic medications are organized by their neurotransmitter targets: SSRIs/SNRIs modulate serotonin and norepinephrine reuptake for depression and anxiety, antipsychotics block D2 receptors (typicals cause EPS on a timeline from dystonia to tardive dyskinesia; atypicals add 5-HT2A blockade with metabolic side effects), mood stabilizers (lithium with its narrow TI, nephrogenic DI, and Ebstein anomaly risk; valproate and carbamazepine with neural tube defects), benzodiazepines enhance GABA-A frequency for acute anxiety but risk fatal withdrawal, and the critical emergencies are serotonin syndrome (clonus, serotonergic drugs) versus NMS (rigidity, dopamine blockade) and TCA overdose (widened QRS, sodium bicarbonate).

bottom of page