top of page

eduo
visual

Biostatistics & Epidemiology
Levels of prevention (primary, secondary, tertiary, quaternary)
Core Principle of Prevention Levels in Medicine
🧷
Prevention in medicine is stratified into distinct levels based on the timing of intervention relative to disease onset and progression.
🧷
Primary prevention occurs before disease develops, secondary prevention detects and treats disease in its early asymptomatic phase, tertiary prevention minimizes complications of established disease, and quaternary prevention protects patients from unnecessary medical interventions.
🧷
This framework guides resource allocation, screening program development, and clinical decision-making across all medical specialties.
🧷
Understanding prevention levels is essential for both population health management and individual patient care decisions.

Primary Prevention: Stopping Disease Before It Starts
📍
Primary prevention targets risk factors and exposures before any pathological process begins, aiming to reduce disease incidence in the population.
📍
Classic examples include vaccination programs, water fluoridation, seat belt laws, smoking cessation counseling, and dietary modifications to prevent cardiovascular disease.
📍
The intervention occurs during the pre-pathogenesis period when individuals are healthy and free from the disease of interest.
📍
Board pearl: If a question describes an intervention in healthy individuals to prevent future disease occurrence, it represents primary prevention regardless of the specific method used.

Mechanisms and Examples of Primary Prevention
🔹
Immunizations create immunity before pathogen exposure: MMR vaccine prevents measles, HPV vaccine prevents cervical cancer, hepatitis B vaccine prevents chronic liver disease and hepatocellular carcinoma.
🔹
Lifestyle modifications target modifiable risk factors: Mediterranean diet to prevent cardiovascular disease, weight-bearing exercise to prevent osteoporosis, sunscreen use to prevent melanoma.
🔹
Environmental interventions remove hazardous exposures: lead paint removal, asbestos abatement, workplace safety regulations.
🔹
Chemoprevention uses medications in at-risk populations: aspirin for cardiovascular disease, statins for hyperlipidemia, folate supplementation to prevent neural tube defects.

Secondary Prevention: Early Detection and Treatment
⭐
Secondary prevention identifies disease in its asymptomatic or early symptomatic phase when treatment is most effective, aiming to reduce disease prevalence and severity.
⭐
The hallmark of secondary prevention is screening — systematically testing asymptomatic individuals to detect disease before clinical manifestations appear.
⭐
Successful secondary prevention requires that early detection and treatment improve outcomes compared to waiting for symptomatic presentation.
⭐
Board pearl: Screening tests (mammography, colonoscopy, Pap smear) are always secondary prevention when applied to asymptomatic individuals, even if they prevent progression to invasive cancer.

Criteria for Effective Screening Programs
✅
The Wilson-Jungner criteria guide screening program development: important health problem, accepted treatment available, facilities for diagnosis and treatment, recognizable latent stage, suitable test, test acceptable to population, natural history understood, agreed policy on whom to treat, cost-effectiveness, and continuous case-finding.
✅
The disease must have a detectable preclinical phase during which intervention improves outcomes — this window between detectability and symptoms is the critical screening period.
✅
Lead time bias, length bias, and overdiagnosis are inherent challenges that must be considered when evaluating screening effectiveness.
✅
Board distinction: A good screening test prioritizes sensitivity (missing few cases) over specificity (confirming diagnosis comes later).

Classic Secondary Prevention Examples
🧠
Cancer screening: mammography for breast cancer (age 50-74), colonoscopy for colorectal cancer (age 45-75), low-dose CT for lung cancer in high-risk smokers, Pap smear for cervical cancer.
🧠
Cardiovascular screening: blood pressure measurement for hypertension, lipid panels for dyslipidemia, abdominal ultrasound for AAA in male smokers over 65.
🧠
Infectious disease screening: tuberculin skin testing in high-risk populations, HIV screening in all adults, hepatitis C screening in baby boomers.
🧠
Metabolic screening: fasting glucose or HbA1c for diabetes, TSH for thyroid disease, DEXA scan for osteoporosis in postmenopausal women.

Tertiary Prevention: Minimizing Impact of Established Disease
⚡
Tertiary prevention focuses on individuals with symptomatic disease, aiming to slow progression, prevent complications, restore function, and improve quality of life.
⚡
Unlike primary and secondary prevention which target disease incidence and early detection, tertiary prevention accepts that disease is present and works to optimize outcomes.
⚡
Rehabilitation, disease management programs, and complication screening in chronic disease all represent tertiary prevention strategies.
⚡
Board pearl: Any intervention in a patient with diagnosed disease aimed at preventing complications or deterioration is tertiary prevention, regardless of the specific approach.

Tertiary Prevention Strategies and Examples
📌
Diabetes management: glycemic control to prevent retinopathy, nephropathy, and neuropathy; foot exams to prevent amputations; ACE inhibitors for nephroprotection.
📌
Post-MI care: cardiac rehabilitation, beta-blockers and ACE inhibitors to prevent remodeling, antiplatelet therapy to prevent recurrent events, lifestyle modification programs.
📌
Stroke rehabilitation: physical therapy to regain function, speech therapy for aphasia, occupational therapy for activities of daily living, secondary stroke prevention with antithrombotics.
📌
Mental health: psychosocial rehabilitation for schizophrenia, relapse prevention in substance use disorders, medication adherence programs in bipolar disorder.

Quaternary Prevention: Protecting Patients from Medical Harm
📣
Quaternary prevention, the newest addition to the prevention framework, protects patients from unnecessary, excessive, or harmful medical interventions.
📣
This level addresses the growing problem of overdiagnosis, overtreatment, and medicalization of normal life processes that can cause net harm to patients.
📣
Examples include avoiding unnecessary imaging that leads to incidental findings, preventing polypharmacy in elderly patients, and resisting aggressive screening in limited life expectancy.
📣
Board pearl: Quaternary prevention is particularly relevant in elderly patients where the harms of intervention may outweigh benefits due to competing mortality risks.

Distinguishing Prevention Levels in Complex Scenarios
🔸
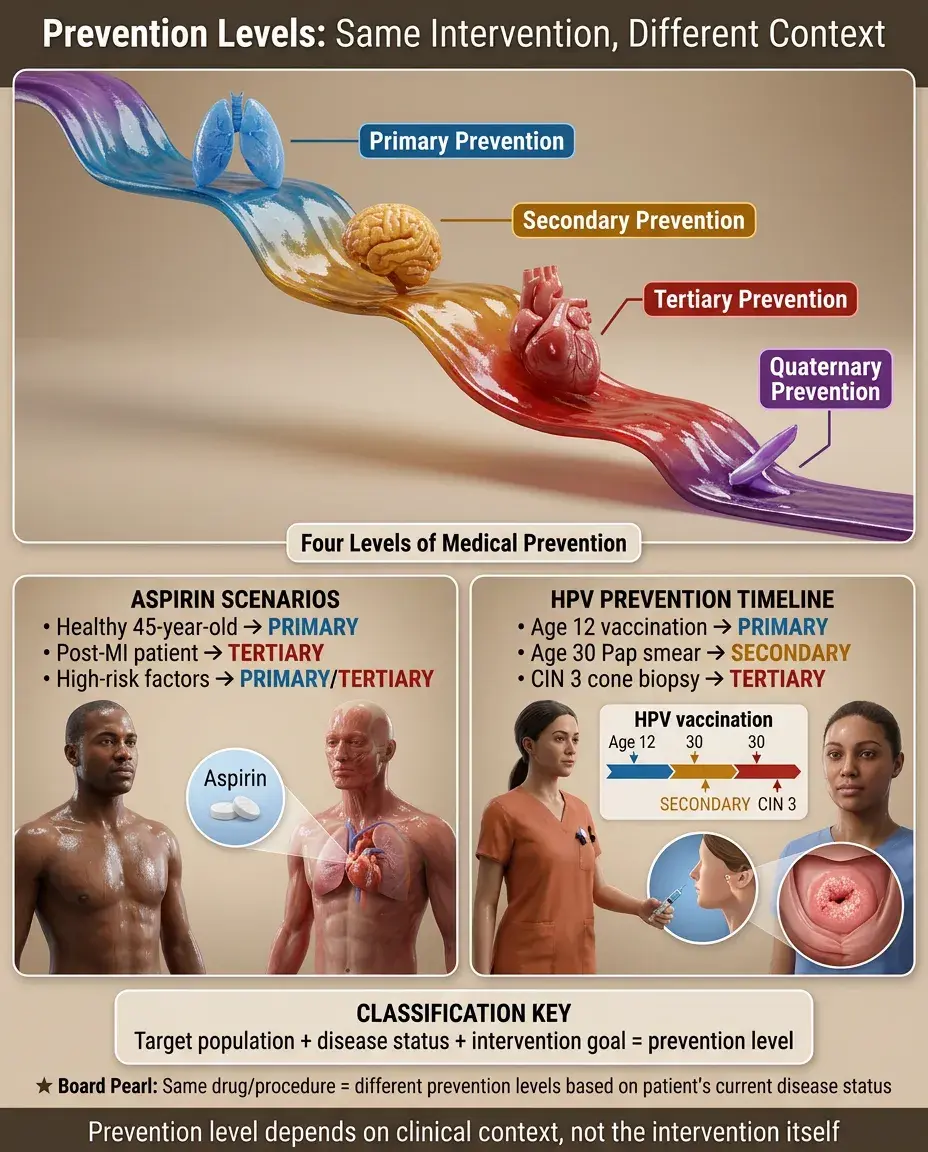
Some interventions blur boundaries between prevention levels — understanding the primary goal and target population clarifies classification.
🔸
Aspirin in a patient with no cardiovascular disease = primary prevention; aspirin after first MI = tertiary prevention; aspirin in asymptomatic patient with multiple risk factors = may be considered either.
🔸
HPV vaccination in a 12-year-old = primary prevention; Pap smear in a 30-year-old = secondary prevention; cone biopsy for CIN 3 = tertiary prevention.
🔸
Board distinction: The same intervention can represent different prevention levels depending on the clinical context and patient's disease status.
Population Health and Prevention Strategies
🧷
Primary prevention typically offers the greatest population health benefit by reducing disease incidence, but requires treating many to benefit few (high number needed to treat).
🧷
Secondary prevention effectiveness depends on test characteristics, disease prevalence, and availability of effective early treatment — works best for slowly progressive diseases with long asymptomatic phases.
🧷
Tertiary prevention provides the most immediate individual benefit but affects only those already diseased, limiting population impact.
🧷
Resource allocation must balance prevention levels: vaccines (primary) vs. screening programs (secondary) vs. disease management (tertiary).

Lead Time and Length Time Bias in Screening
📍
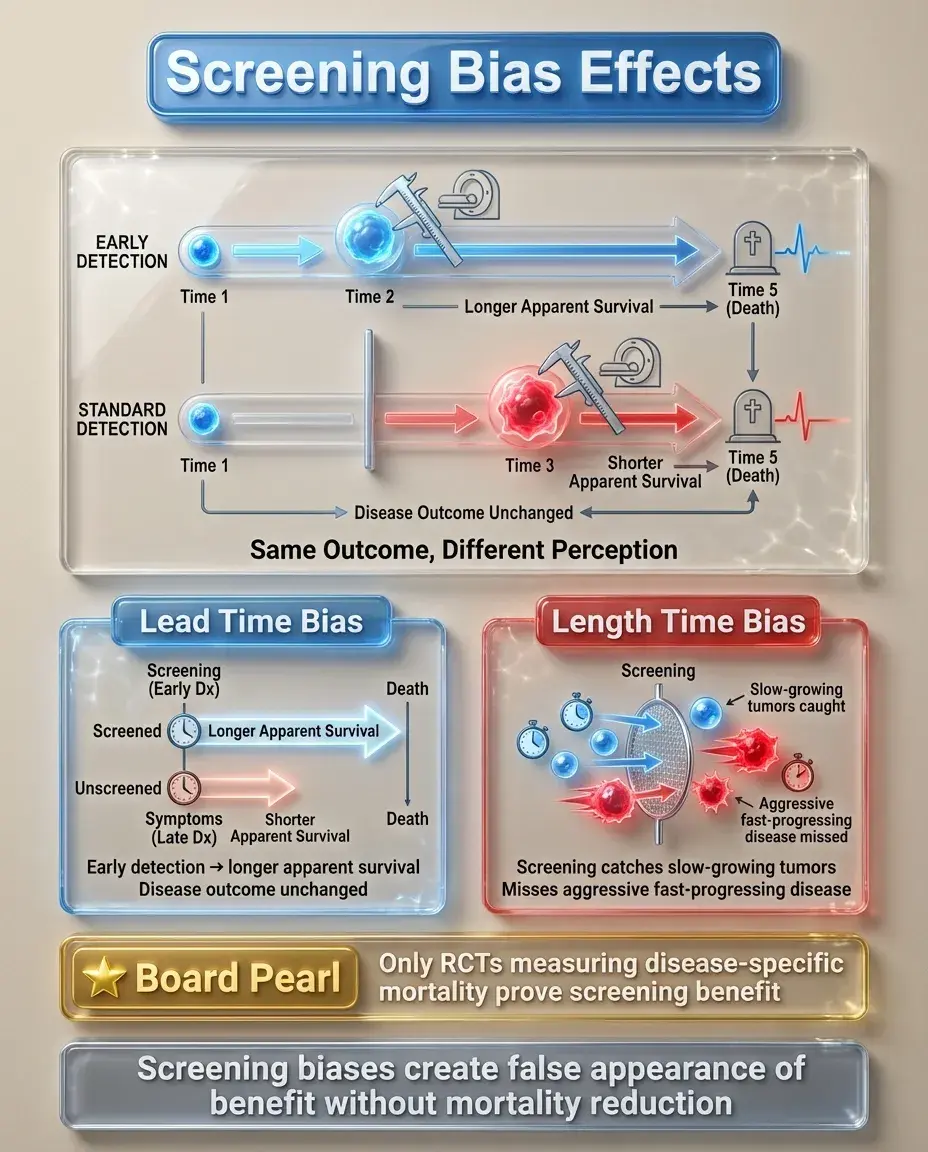
Lead time bias occurs when screening detects disease earlier without changing the outcome — survival appears longer simply because diagnosis occurred earlier in the disease course.
📍
Length time bias occurs because screening preferentially detects slower-growing, less aggressive diseases with longer asymptomatic phases, making screening appear more effective than it actually is.
📍
These biases can make screening programs appear beneficial even when they don't reduce disease-specific mortality.
📍
Board pearl: The only way to prove screening effectiveness while avoiding these biases is through randomized controlled trials measuring disease-specific mortality, not survival from diagnosis.
Overdiagnosis and Overtreatment
🔹
Overdiagnosis occurs when screening detects abnormalities that would never have caused symptoms or death during the patient's lifetime — particularly problematic in cancer screening.
🔹
Prostate cancer screening with PSA exemplifies this issue: many detected cancers would never progress to clinical significance, but treatment causes morbidity.
🔹
Thyroid cancer incidence has increased dramatically due to incidental detection on imaging, while mortality remains unchanged — classic overdiagnosis pattern.
🔹
Quaternary prevention specifically addresses this by promoting thoughtful screening practices and shared decision-making about testing.

Prevention Levels in Special Populations
⭐
Elderly patients: Primary prevention benefits decrease with shortened life expectancy; screening (secondary prevention) should consider life expectancy vs. time to benefit; quaternary prevention becomes increasingly important.
⭐
Immunocompromised patients: Enhanced primary prevention through additional vaccines; modified screening protocols for opportunistic infections; aggressive tertiary prevention of complications.
⭐
Pregnancy: Primary prevention through prenatal vitamins; secondary prevention via prenatal screening; tertiary prevention of pregnancy complications.
⭐
Board distinction: Prevention strategies must be individualized based on life expectancy, comorbidities, and patient values.

Economic Considerations in Prevention
✅
Primary prevention through population-level interventions (water fluoridation, clean air laws) typically offers the best cost-effectiveness by preventing disease in many individuals.
✅
Secondary prevention cost-effectiveness depends on disease prevalence, test costs, and treatment effectiveness — screening high-risk groups improves efficiency.
✅
Tertiary prevention can be expensive per individual but may reduce overall costs by preventing costly complications and hospitalizations.
✅
Board pearl: Cost-effectiveness analysis uses quality-adjusted life years (QALYs) to compare prevention strategies — interventions <$50,000/QALY are generally considered cost-effective.

Prevention Paradox and Rose's Strategy
🧠
The prevention paradox: interventions that provide large population benefits may offer little to each participating individual, while high-risk strategies benefit individuals greatly but have limited population impact.
🧠
Population strategy (Rose): small risk reductions across entire populations yield large absolute benefits — reducing average blood pressure by 5 mmHg prevents more strokes than treating only severe hypertension.
🧠
High-risk strategy: intensive interventions in those most likely to benefit — provides larger individual benefit but misses the majority of cases that arise from the moderate-risk majority.
🧠
Effective prevention programs often combine both strategies.

Natural History and Critical Points for Intervention
⚡
Understanding disease natural history identifies optimal intervention windows: biological onset → subclinical disease → clinical symptoms → outcomes.
⚡
Primary prevention targets the period before biological onset by modifying risk factors and exposures.
⚡
Secondary prevention exploits the detectable preclinical phase between biological onset and symptoms.
⚡
Tertiary prevention intervenes after symptoms appear to prevent progression to adverse outcomes.
⚡
Board pearl: The effectiveness of each prevention level depends on the duration and detectability of each disease phase.

Implementation Challenges Across Prevention Levels
📌
Primary prevention challenges: long time horizons to see benefits, difficulty maintaining adherence to lifestyle changes, vaccine hesitancy, need for population-wide implementation.
📌
Secondary prevention challenges: false positives causing anxiety and further testing, overdiagnosis, ensuring equal access to screening, managing incidental findings.
📌
Tertiary prevention challenges: medication adherence, care coordination across specialists, patient engagement in self-management, addressing social determinants affecting disease control.
📌
Quaternary prevention challenges: changing medical culture that rewards doing more, patient expectations for testing and treatment, medicolegal concerns.

Board Question Stem Patterns
📣
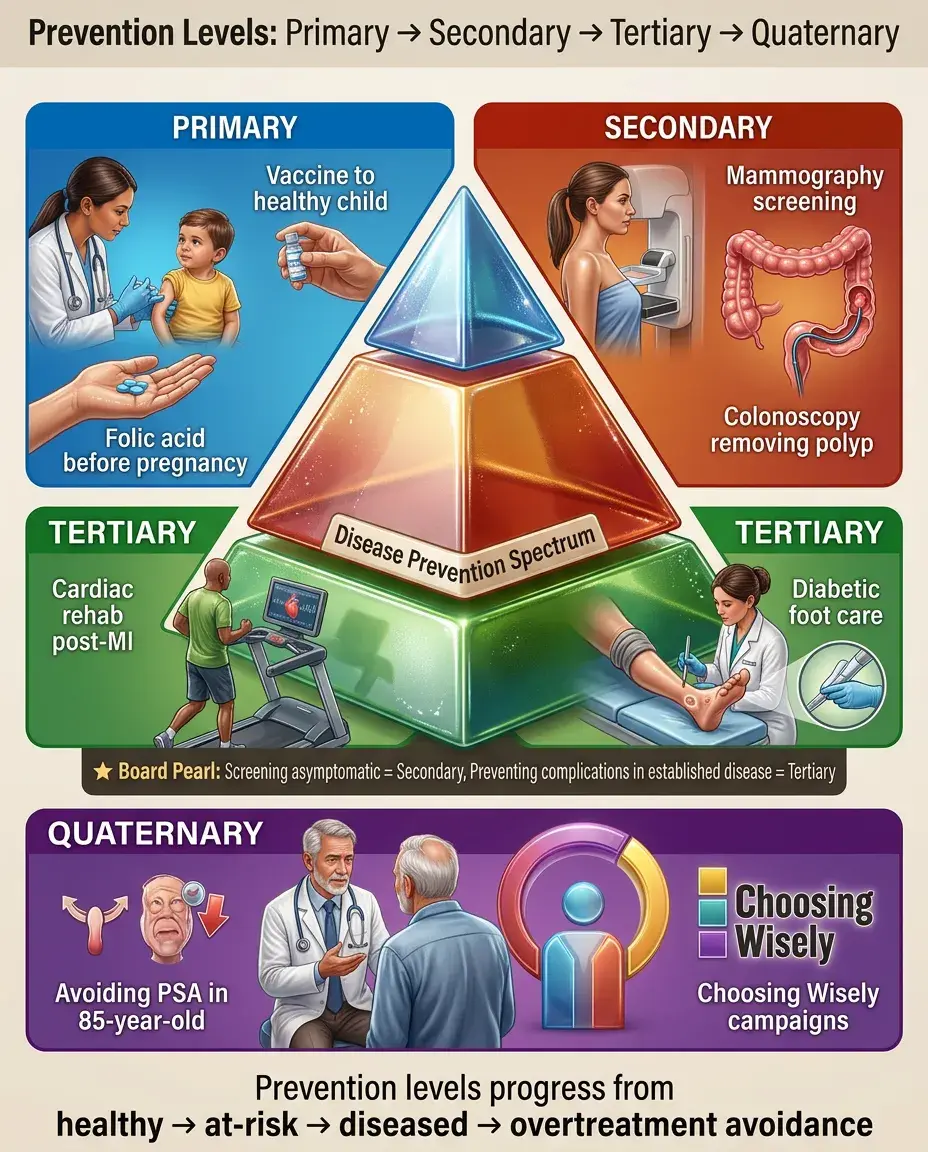
Vaccine given to healthy children → primary prevention.
📣
Screening test in asymptomatic individual → secondary prevention.
📣
Intervention in patient with established disease to prevent complications → tertiary prevention.
📣
Avoiding PSA screening in 85-year-old man → quaternary prevention.
📣
Mammography detecting DCIS → secondary prevention (even though preventing invasive cancer).
📣
Cardiac rehab after MI → tertiary prevention.
📣
Folic acid in woman planning pregnancy → primary prevention.
📣
Choosing Wisely campaign recommendations → quaternary prevention.
📣
Colonoscopy removing adenomatous polyp → secondary prevention.
One-Line Recap
🔸
Prevention levels progress from primary (preventing disease occurrence through risk factor modification), to secondary (detecting asymptomatic disease via screening), to tertiary (minimizing complications in established disease), to quaternary (protecting patients from harmful medical interventions), with each level requiring different strategies, target populations, and outcome measures for optimal individual and population health impact.

bottom of page