top of page

eduo
visual

Integumentary system
Impetigo, cellulitis, herpes, dermatophytes, scabies
Core Principle of Common Skin and Soft Tissue Infections
🧷
Skin infections are classified by depth of involvement: superficial (epidermis only), superficial dermal (epidermis + papillary dermis), deep dermal/subcutaneous (reticular dermis + fat), and systemic spread.
🧷
Each infection has a characteristic morphology, causative organism, and distribution pattern that allows clinical diagnosis without culture in most cases.
🧷
The skin's barrier function is compromised by breaks (trauma, eczema, IV drug use), moisture (intertriginous areas), and immunosuppression — creating entry points for pathogens.
🧷
Board pearl: Match the morphology to the organism: honey-crusted lesions → Staph aureus, serpentine tracks → scabies, annular scaly plaques → dermatophytes, grouped vesicles on erythematous base → HSV.

Impetigo: The Superficial Bacterial Infection
📍
Impetigo is a highly contagious superficial infection of the epidermis caused by Staphylococcus aureus (most common) or Streptococcus pyogenes (Group A strep).
📍
Two forms: nonbullous (70%) presents with honey-colored crusts on erythematous base; bullous (30%) presents with fragile fluid-filled bullae that rupture leaving collarettes of scale.
📍
Predilection for face and extremities, especially around nose and mouth in children. Spread by direct contact and fomites.
📍
Bullous impetigo is always S. aureus due to exfoliative toxins A and B that cleave desmoglein-1 in the superficial epidermis.
📍
Board pearl: Honey-crusted lesions in a child = impetigo until proven otherwise.

Cellulitis: The Deep Dermal Infection
🔹
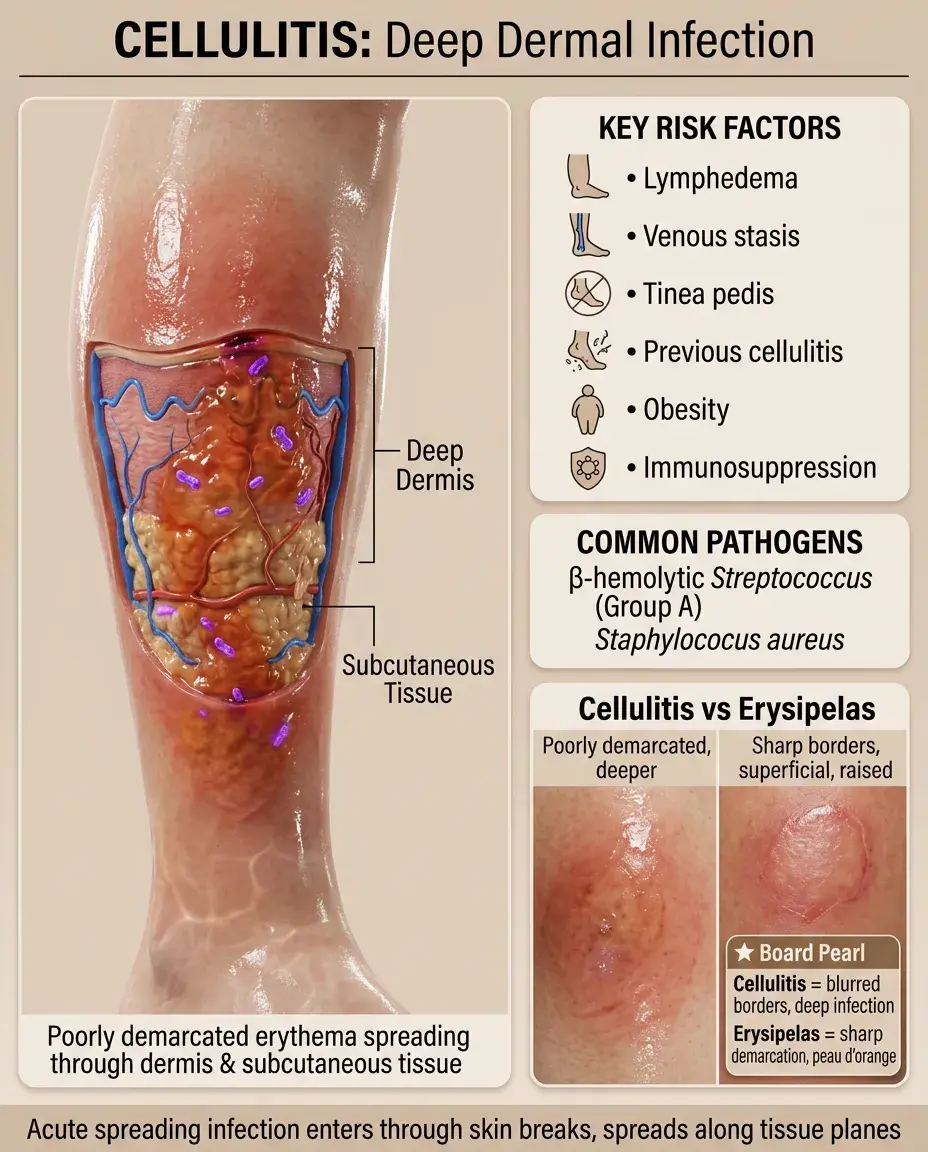
Cellulitis is an acute spreading infection of the dermis and subcutaneous tissue, presenting as poorly demarcated erythema, warmth, edema, and tenderness.
🔹
Most commonly caused by β-hemolytic streptococci (especially Group A) and S. aureus entering through breaks in skin barrier.
🔹
Risk factors: lymphedema, venous stasis, obesity, tinea pedis (creates portal of entry), previous cellulitis, immunosuppression.
🔹
Spreads along tissue planes with indistinct borders — unlike erysipelas which has sharp demarcation and involves superficial dermis only.
🔹
Board distinction: Cellulitis = poorly demarcated, deeper infection; Erysipelas = sharply demarcated, raised, superficial infection with peau d'orange appearance.
Special Cellulitis Scenarios
⭐
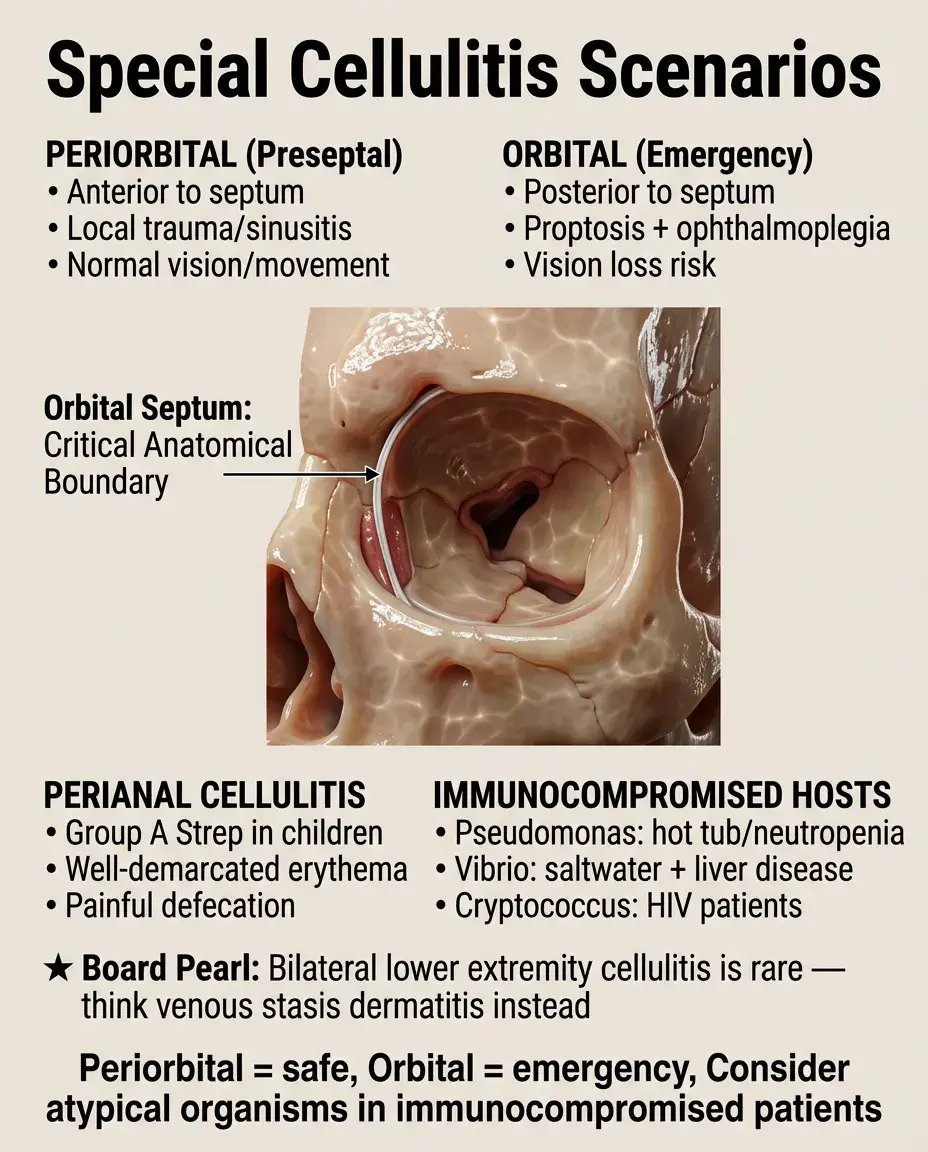
Periorbital (preseptal) cellulitis: anterior to orbital septum, usually from local trauma or spread from sinusitis. No vision changes or eye movement restriction.
⭐
Orbital cellulitis: posterior to septum, medical emergency with proptosis, ophthalmoplegia, vision loss. Requires immediate CT and IV antibiotics.
⭐
Perianal cellulitis in children: Group A strep, presents with well-demarcated perianal erythema and painful defecation.
⭐
Board pearl: Cellulitis in immunocompromised hosts → consider atypical organisms: Pseudomonas (hot tub exposure, neutropenia), Vibrio vulnificus (saltwater exposure, liver disease), Cryptococcus (HIV).
⭐
Bilateral lower extremity cellulitis is rare — consider venous stasis dermatitis instead.
Herpes Simplex Virus: The Vesicular Eruption
✅
HSV-1 (predominantly orofacial) and HSV-2 (predominantly genital) cause recurrent vesicular eruptions on an erythematous base.
✅
Primary infection: extensive painful vesicles, systemic symptoms, lymphadenopathy. Recurrent infection: limited vesicles preceded by prodromal tingling.
✅
Pathophysiology: virus enters through mucosa → replicates in epithelial cells → travels retrograde to dorsal root ganglia where it establishes latency.
✅
Reactivation triggers: UV light, stress, immunosuppression, trauma, fever ("fever blisters").
✅
Board pearl: Grouped vesicles on erythematous base = HSV. Tzanck smear shows multinucleated giant cells but cannot distinguish HSV from VZV.

HSV Clinical Presentations and Complications
🧠
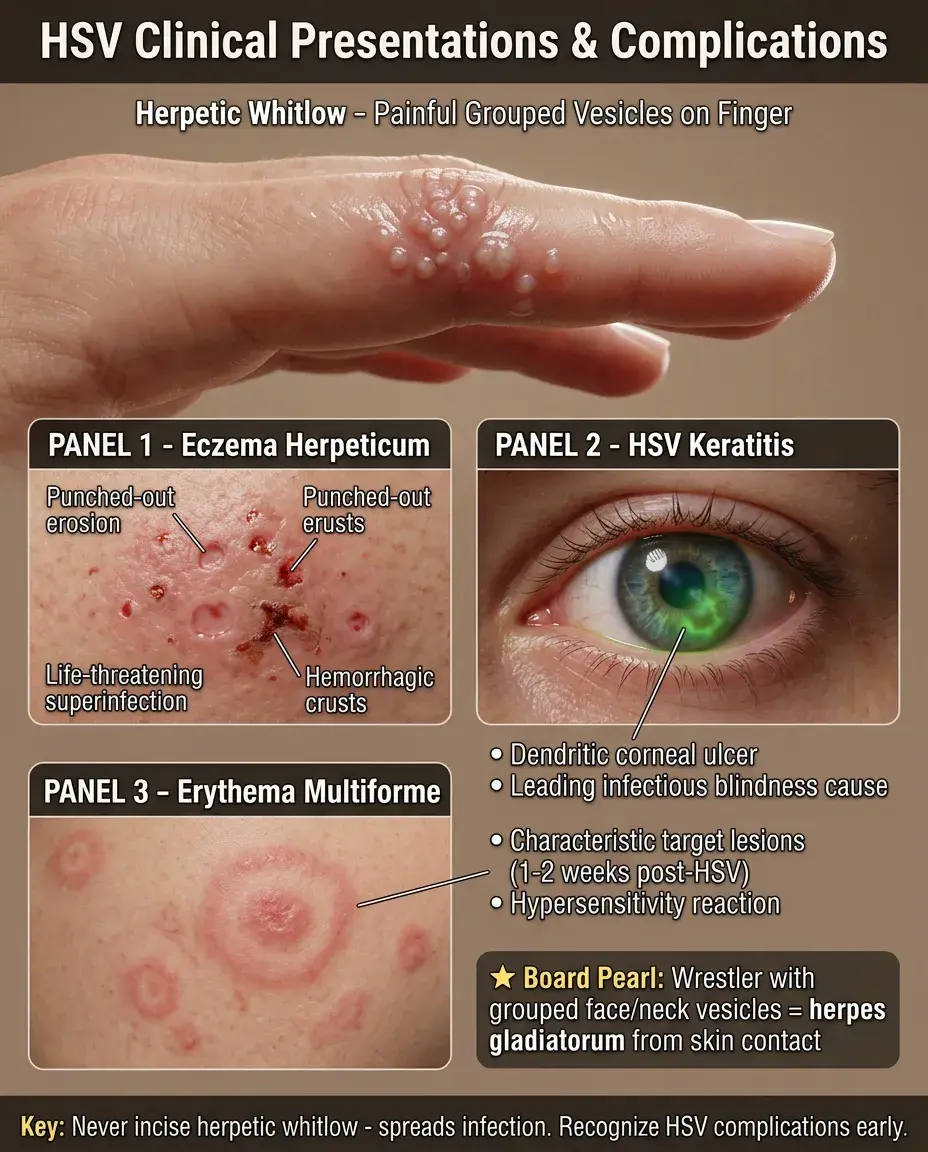
Herpetic whitlow: painful vesicles on finger, common in healthcare workers and children who suck thumbs. Do not incise — risk of spreading infection.
🧠
Eczema herpeticum: HSV superinfection of atopic dermatitis, presents with punched-out erosions and hemorrhagic crusts. Can be life-threatening.
🧠
HSV keratitis: dendritic corneal ulcer seen with fluorescein staining. Leading infectious cause of corneal blindness.
🧠
Erythema multiforme: target lesions appearing 1-2 weeks after HSV outbreak, represents hypersensitivity reaction.
🧠
Board pearl: Wrestler or rugby player with grouped vesicles on face/neck = herpes gladiatorum from skin-to-skin contact.
Dermatophyte Basics: The Fungal Infections
⚡
Dermatophytes are fungi that invade and proliferate in keratinized tissue (stratum corneum, hair, nails) but cannot penetrate viable tissue.
⚡
Three genera: Trichophyton (most common), Microsporum, Epidermophyton. Named by body site: tinea capitis (scalp), corporis (body), pedis (feet), etc.
⚡
Transmission via direct contact, fomites, or autoinoculation. Thrives in warm, moist environments.
⚡
Classic morphology: annular (ring-shaped) plaques with central clearing and active scaly border that contains the advancing fungi.
⚡
Board pearl: KOH prep of scale from active border shows branching hyphae crossing dermatophyte. Wood's lamp only fluoresces certain Microsporum species.

Tinea Infections by Location
📌
Tinea capitis: scalp infection in children, presents as patchy alopecia with scale. Kerion = boggy tender plaque with pustules (severe inflammatory type).
📌
Tinea corporis: "ringworm" on body with classic annular morphology. Pet exposure suggests Microsporum canis.
📌
Tinea pedis: "athlete's foot" with three patterns — interdigital (most common), moccasin (dry, scaly), vesiculobullous (blisters).
📌
Tinea cruris: "jock itch" in groin folds, spares scrotum (unlike candida which involves scrotum).
📌
Tinea versicolor: actually caused by Malassezia (not a true dermatophyte), presents as hypo- or hyperpigmented macules with fine scale.
📌
Board distinction: Tinea cruris spares scrotum; Candida involves scrotum.

Onychomycosis and Tinea Complications
📣
Onychomycosis: dermatophyte nail infection causing yellow-brown discoloration, thickening, subungual debris, and onycholysis (nail separation).
📣
Trichophyton rubrum causes 90% of cases. Toenails affected more than fingernails due to slower growth and occlusive footwear.
📣
Complications: secondary bacterial infection through fissured skin, especially in diabetics who may develop cellulitis.
📣
Majocchi's granuloma: deep dermatophyte infection of hair follicles forming nodules, often from shaving legs with tinea.
📣
Board pearl: Tinea + id reaction = dermatophytid, a hypersensitivity eruption at distant site (vesicles on palms from tinea pedis).

Scabies: The Intensely Pruritic Infestation
🔸
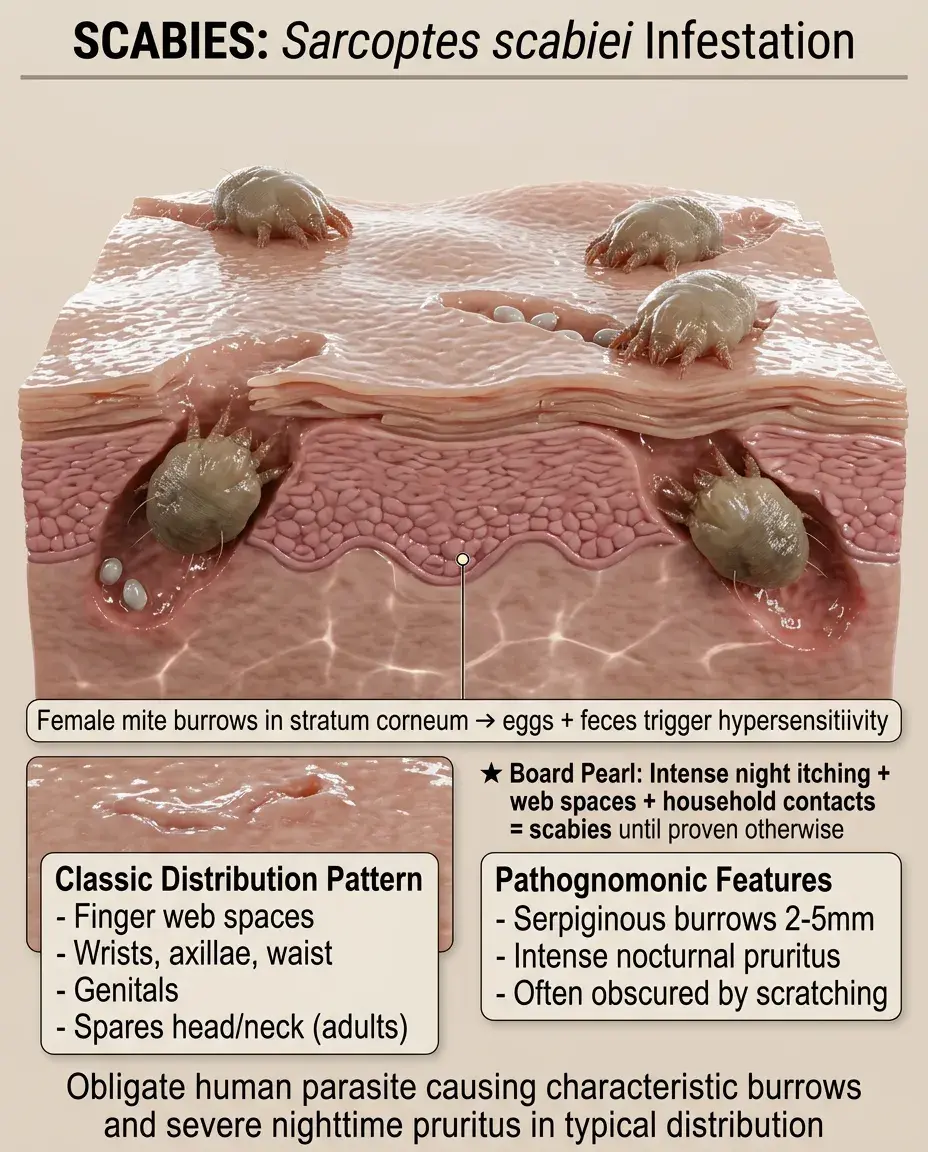
Caused by Sarcoptes scabiei var. hominis, an obligate human parasite mite that burrows into the stratum corneum.
🔸
Female mite burrows and lays eggs → hypersensitivity reaction to mites, eggs, and feces causes intense pruritus worst at night.
🔸
Classic distribution: finger web spaces, wrists, axillae, waist, genitals. Spares head and neck in adults (but not in infants).
🔸
Pathognomonic sign: serpiginous burrows 2-5mm long, but often obscured by excoriation.
🔸
Board pearl: Intense nocturnal pruritus + web space involvement + household contacts with similar symptoms = scabies until proven otherwise.
Scabies Variants and Diagnosis
🧷
Classic scabies: 10-15 mites per person, typical burrows and papules with excoriations.
🧷
Crusted (Norwegian) scabies: thousands of mites in hyperkeratotic crusts, seen in immunocompromised. Highly contagious but less pruritic.
🧷
Nodular scabies: persistent reddish-brown nodules in covered areas (axillae, groin, buttocks) that persist after treatment.
🧷
Diagnosis: microscopy of skin scraping with mineral oil shows mites, eggs, or fecal pellets (scybala). Low sensitivity but high specificity.
🧷
Board pearl: Persistent nodules after scabies treatment represent hypersensitivity reaction, not active infection — treat with topical steroids.

Treatment Principles for Bacterial Infections
📍
Impetigo: topical mupirocin for limited disease, oral antibiotics (cephalexin, dicloxacillin) for extensive disease or multiple lesions.
📍
Cellulitis: oral antibiotics covering strep and staph (cephalexin, dicloxacillin). Add MRSA coverage (TMP-SMX, doxycycline) if risk factors.
📍
Severe cellulitis or systemic signs: IV antibiotics (cefazolin, nafcillin). Add vancomycin for MRSA coverage.
📍
Duration: impetigo 7 days, cellulitis 5-10 days depending on response.
📍
Board pearl: Failure to improve after 48-72 hours of appropriate antibiotics → consider abscess, necrotizing fasciitis, or non-infectious mimic.
Treatment Principles for Viral and Fungal Infections
🔹
HSV: oral antivirals (acyclovir, valacyclovir, famciclovir) shorten duration if started within 72 hours. Suppressive therapy for frequent recurrences.
🔹
Severe HSV (eczema herpeticum, disseminated): IV acyclovir.
🔹
Tinea corporis/cruris: topical antifungals (terbinafine, azoles) for 2-4 weeks, continuing 1 week after clearance.
🔹
Tinea capitis/onychomycosis: requires systemic therapy (terbinafine, itraconazole) due to hair/nail involvement.
🔹
Board pearl: Tinea capitis always requires oral therapy — topical agents cannot penetrate hair shaft.

Scabies Treatment and Environmental Measures
⭐
First-line: permethrin 5% cream applied neck down (include head in infants), left on 8-14 hours, repeat in 1 week.
⭐
Alternative: oral ivermectin, especially for crusted scabies or treatment failure. Not approved in pregnancy or children <15kg.
⭐
All household contacts and sexual partners must be treated simultaneously regardless of symptoms.
⭐
Environmental: wash clothing and bedding in hot water, seal non-washables in plastic bags for 72 hours (mites die off human host).
⭐
Board pearl: Pruritus may persist 2-4 weeks after successful treatment due to dead mite antigens — not treatment failure.

Complications and Secondary Infections
✅
Post-streptococcal glomerulonephritis: can follow impetigo caused by nephritogenic strains of Group A strep. Presents 1-2 weeks later with hematuria, edema.
✅
Lymphangitis: red streaks along lymphatics from cellulitis site, indicates spreading infection.
✅
Bacteremia: especially with facial cellulitis or immunocompromised hosts. Blood cultures indicated for severe disease.
✅
Impetiginization: secondary bacterial infection of any dermatosis (eczema, insect bites, HSV) creating honey-crusted lesions.
✅
Board pearl: Unlike pharyngitis, skin infections with Group A strep can cause PSGN but not rheumatic fever.

Differential Diagnosis Pitfalls
🧠
"Cellulitis" that's bilateral → likely stasis dermatitis (also warm, red, but with scaling and chronic changes).
🧠
"Ringworm" on face that doesn't respond to antifungals → consider lupus (annular erythematous plaques) or granuloma annulare.
🧠
"Impetigo" in adults that keeps recurring → consider pemphigus foliaceus or IgA pemphigus.
🧠
"HSV" with dermatomal distribution → herpes zoster (shingles).
🧠
"Scabies" in a clean patient → consider neurotic excoriations, but remember scabies affects all socioeconomic groups.
🧠
Board distinction: Bullous impetigo vs pemphigus: both have flaccid bullae, but pemphigus has positive Nikolsky sign and oral involvement.

Risk Factors and Prevention
⚡
Impetigo: daycare attendance, poor hygiene, minor trauma, preexisting dermatitis. Prevention: handwashing, avoid sharing towels.
⚡
Cellulitis: lymphedema, chronic venous insufficiency, obesity, diabetes, tinea pedis. Prevention: treat predisposing conditions, daily skin care.
⚡
HSV: immunosuppression increases frequency and severity. Prevention: avoid contact during outbreaks, suppressive therapy for frequent recurrences.
⚡
Dermatophytes: occlusive footwear, shared showers, pet exposure. Prevention: keep feet dry, wear shower shoes, treat infected pets.
⚡
Scabies: overcrowding, institutional settings. Prevention: avoid skin-to-skin contact, prompt treatment of cases.

Immunocompromised Host Considerations
📌
HIV: chronic HSV ulcers >1 month is AIDS-defining. Crusted scabies more common. Tinea may be extensive and treatment-resistant.
📌
Transplant patients: any cellulitis can rapidly progress. HSV prophylaxis often needed. Atypical organisms more common.
📌
Neutropenia: ecthyma gangrenosum (Pseudomonas), rapid progression to bacteremia.
📌
Diabetes: malignant otitis externa (Pseudomonas), rhinocerebral mucormycosis, severe cellulitis with gas-forming organisms.
📌
Board pearl: Necrotic skin lesion with green-black eschar in neutropenic patient = ecthyma gangrenosum (Pseudomonas) until proven otherwise.

Board Question Stem Patterns
📣
Honey-crusted lesions on child's face → impetigo (S. aureus or Group A strep).
📣
Painful grouped vesicles preceded by tingling → HSV.
📣
Annular scaly plaque with central clearing → tinea corporis.
📣
Intense nocturnal pruritus with web space papules → scabies.
📣
Rapidly spreading erythema with fever after minor trauma → cellulitis.
📣
Wrestler with boggy scalp plaque and hair loss → kerion (severe tinea capitis).
📣
Eczematous child with punched-out erosions and fever → eczema herpeticum.
📣
Red, hot, swollen leg that's bilateral → stasis dermatitis, not cellulitis.

One-Line Recap
🔸
Common skin infections are diagnosed by morphology and distribution: honey-crusted lesions (impetigo), poorly demarcated deep erythema (cellulitis), grouped vesicles (HSV), annular scaly plaques (dermatophytes), and intensely pruritic papules in web spaces (scabies) — each with specific treatment approaches and potential complications that become board question fodder.

bottom of page