top of page

eduo
visual

Reproductive & Endocrine Systems
Hyperaldosteronism
Core Principle of Hyperaldosteronism
🧷
Hyperaldosteronism is excessive aldosterone production causing sodium retention, potassium wasting, and hypertension through enhanced Na⁺/K⁺ exchange in the distal nephron.
🧷
Primary hyperaldosteronism (Conn syndrome) arises from autonomous adrenal production — aldosterone-producing adenoma or bilateral adrenal hyperplasia — with suppressed renin.
🧷
Secondary hyperaldosteronism results from physiologic renin-angiotensin-aldosterone system (RAAS) activation due to renal hypoperfusion, with both renin and aldosterone elevated.
🧷
The key diagnostic distinction: primary has high aldosterone with low renin; secondary has high aldosterone with high renin.

Aldosterone Physiology and Actions
📍
Aldosterone binds mineralocorticoid receptors in principal cells of the collecting duct, upregulating epithelial sodium channels (ENaC) and Na⁺/K⁺-ATPase pumps.
📍
This promotes Na⁺ reabsorption and K⁺ secretion, with water following sodium osmotically → volume expansion and hypertension.
📍
Aldosterone also stimulates H⁺-ATPase in intercalated cells → H⁺ excretion and metabolic alkalosis.
📍
Normal regulation: angiotensin II and hyperkalemia stimulate aldosterone; hypokalemia and atrial natriuretic peptide inhibit it.
📍
Board pearl: The triad of hypertension, hypokalemia, and metabolic alkalosis should immediately trigger consideration of hyperaldosteronism.

Primary Hyperaldosteronism: Causes and Epidemiology
🔹
Aldosterone-producing adenoma (Conn syndrome proper): 35% of cases, typically unilateral, more common in younger patients (30–50 years).
🔹
Bilateral idiopathic hyperplasia: 60% of cases, more common in older patients, rarely amenable to surgical cure.
🔹
Rare causes: unilateral adrenal hyperplasia, aldosterone-producing carcinoma, familial hyperaldosteronism types I–IV.
🔹
Primary hyperaldosteronism accounts for 5–10% of all hypertension and up to 20% of resistant hypertension (uncontrolled on ≥3 medications).
🔹
Board clue: Young patient with severe hypertension and spontaneous hypokalemia → think aldosterone-producing adenoma.

Clinical Presentation of Primary Hyperaldosteronism
⭐
Most patients are asymptomatic and diagnosed during hypertension workup — hypokalemia is present in only 30–50% at diagnosis.
⭐
When symptomatic: muscle weakness, cramping, paresthesias, and polyuria/polydipsia from hypokalemia-induced nephrogenic diabetes insipidus.
⭐
Severe hypokalemia can cause rhabdomyolysis, paralysis, or dangerous arrhythmias.
⭐
Cardiovascular effects exceed those expected from hypertension alone — increased risk of MI, stroke, atrial fibrillation, and LV hypertrophy.
⭐
Board pearl: Absence of hypokalemia does not rule out primary hyperaldosteronism — many patients maintain normal K⁺ with adequate dietary intake.

Secondary Hyperaldosteronism: Mechanisms and Causes
✅
Renal artery stenosis: decreased renal perfusion → renin release → angiotensin II → aldosterone. Classic presentation: resistant hypertension with abdominal bruit.
✅
Heart failure and cirrhosis: decreased effective circulating volume → RAAS activation despite total body volume overload.
✅
Diuretic use: volume depletion and direct stimulation of renin release.
✅
Renin-secreting tumors (juxtaglomerular cell tumors): rare cause in young patients with severe hypertension.
✅
Bartter and Gitelman syndromes: genetic tubulopathies mimicking loop and thiazide diuretics respectively → salt wasting → secondary hyperaldosteronism.

Diagnostic Approach: Initial Screening
🧠
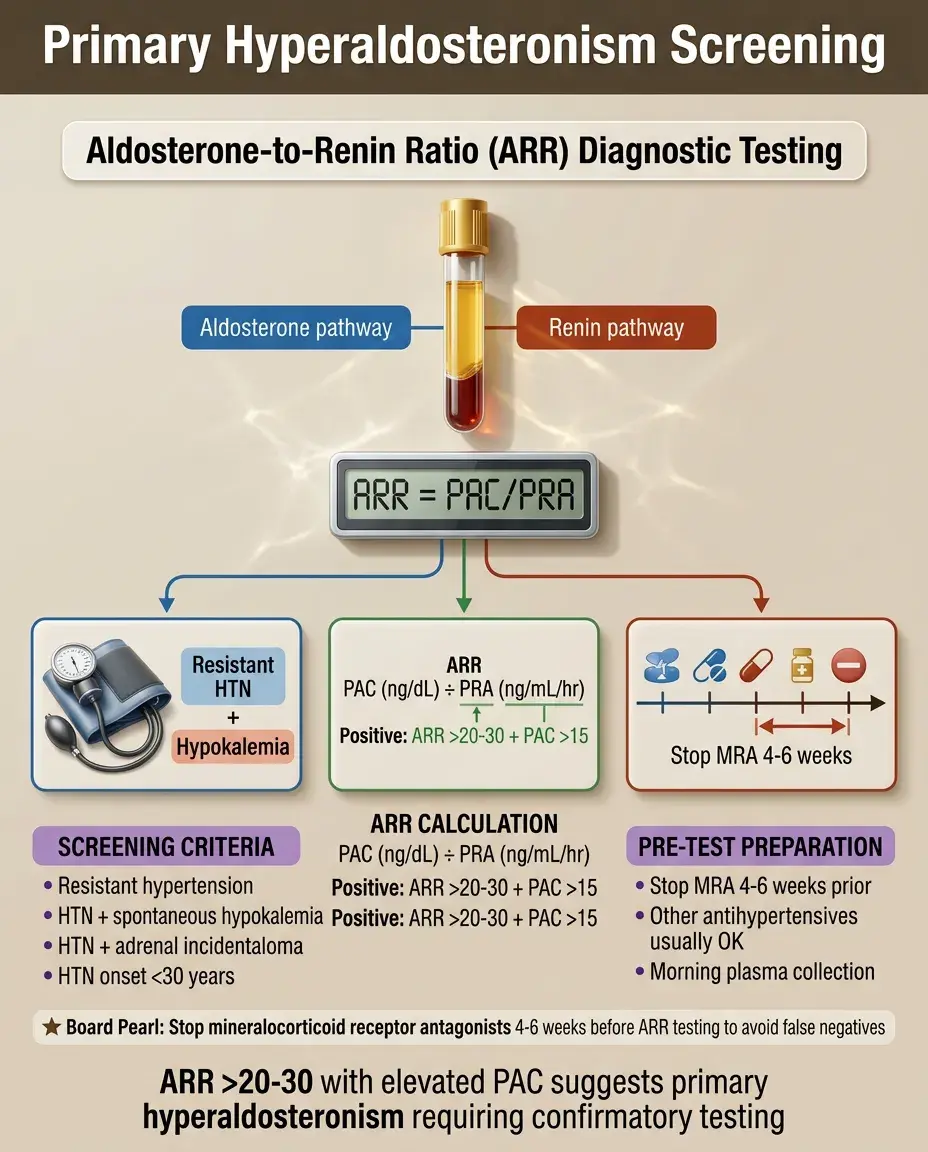
Screen for primary hyperaldosteronism in: resistant hypertension, hypertension with spontaneous or diuretic-induced hypokalemia, hypertension with adrenal incidentaloma, hypertension onset <30 years.
🧠
First step: morning plasma aldosterone concentration (PAC) and plasma renin activity (PRA) or direct renin concentration.
🧠
Calculate aldosterone-to-renin ratio (ARR): PAC (ng/dL) / PRA (ng/mL/hr).
🧠
ARR >20–30 with PAC >15 ng/dL suggests primary hyperaldosteronism.
🧠
Board pearl: Stop mineralocorticoid receptor antagonists 4–6 weeks before testing; other antihypertensives can usually be continued.
Confirmatory Testing for Primary Hyperaldosteronism
⚡
Positive screening requires confirmation with suppression testing — aldosterone should suppress with sodium loading in normal individuals.
⚡
Oral salt loading: high sodium diet (>200 mEq/day) for 3 days followed by 24-hour urine aldosterone. Unsuppressed aldosterone >12 μg/24h confirms diagnosis.
⚡
IV saline suppression: 2L normal saline over 4 hours. Post-infusion aldosterone >10 ng/dL confirms diagnosis.
⚡
Fludrocortisone suppression test: most definitive but rarely used due to complexity.
⚡
Board distinction: In primary hyperaldosteronism, aldosterone fails to suppress with salt loading; in secondary, both renin and aldosterone are appropriately elevated.

Subtype Differentiation: Adenoma vs Hyperplasia
📌
Critical distinction because adenomas are surgically curable while bilateral hyperplasia requires lifelong medical therapy.
📌
Adrenal CT or MRI: initial imaging to identify adenomas (typically <2 cm, unilateral) or bilateral enlargement.
📌
Problem: nonfunctioning incidentalomas are common; imaging alone cannot distinguish functional from nonfunctional masses.
📌
Adrenal venous sampling (AVS): gold standard for lateralization. Aldosterone-to-cortisol ratio >4:1 between sides indicates unilateral disease.
📌
Board pearl: Young patients (<35 years) with unilateral adenoma and marked hyperaldosteronism may proceed to surgery without AVS.

Medical Management Principles
📣
Mineralocorticoid receptor antagonists are first-line: spironolactone (25–100 mg daily) or eplerenone (50–100 mg BID).
📣
Spironolactone: more potent and inexpensive but causes gynecomastia, erectile dysfunction, and menstrual irregularities via antiandrogen effects.
📣
Eplerenone: selective for mineralocorticoid receptor, fewer sexual side effects but less potent and more expensive.
📣
Both drugs risk hyperkalemia — monitor K⁺ and creatinine closely, especially in CKD or with ACE inhibitors/ARBs.
📣
Amiloride (ENaC blocker) is alternative for patients intolerant to MR antagonists.

Surgical Management and Outcomes
🔸
Unilateral adrenalectomy for aldosterone-producing adenoma: 30–60% achieve complete hypertension cure, nearly 100% show improvement.
🔸
Predictors of cure: shorter hypertension duration, fewer antihypertensive medications, younger age, higher preoperative aldosterone.
🔸
Postoperative hypoaldosteronism may occur → monitor for hyperkalemia and salt craving; usually resolves as contralateral adrenal recovers.
🔸
Bilateral adrenalectomy is NOT indicated for bilateral hyperplasia due to lifelong steroid dependence risk.
🔸
Board pearl: Post-adrenalectomy, expect transient hyperkalemia as chronic K⁺ depletion reverses and contralateral suppression resolves.

Familial Hyperaldosteronism Syndromes
🧷
Type I (glucocorticoid-remediable): chimeric CYP11B1/CYP11B2 gene → ACTH regulates aldosterone. Suppressed with dexamethasone. Early-onset hypertension, family history of hemorrhagic stroke.
🧷
Type II: familial clustering of aldosterone-producing adenomas or bilateral hyperplasia. No specific genetic defect identified.
🧷
Type III: KCNJ5 potassium channel mutations → severe early-onset hypertension, massive bilateral adrenal hyperplasia.
🧷
Type IV: CACNA1H calcium channel mutations → childhood-onset hypertension.
🧷
Board clue: Young patient with hypertension that improves with dexamethasone → glucocorticoid-remediable aldosteronism.

Hypokalemia: Mechanisms and Management
📍
Aldosterone-driven K⁺ secretion in collecting duct coupled with increased distal Na⁺ delivery → urinary K⁺ wasting.
📍
Hypokalemia itself perpetuates metabolic alkalosis by promoting H⁺ secretion and HCO₃⁻ retention.
📍
Severe depletion causes muscle weakness, rhabdomyolysis, nephrogenic diabetes insipidus, and cardiac arrhythmias.
📍
K⁺ replacement alone is ineffective without treating underlying hyperaldosteronism — like filling a bucket with a hole.
📍
Board pearl: Refractory hypokalemia despite aggressive replacement → look for ongoing urinary losses from hyperaldosteronism or diuretics.

Metabolic Alkalosis in Hyperaldosteronism
🔹
Aldosterone stimulates H⁺-ATPase in intercalated cells → increased H⁺ secretion → HCO₃⁻ retention → metabolic alkalosis.
🔹
Volume expansion from Na⁺ retention maintains alkalosis by limiting proximal HCO₃⁻ excretion.
🔹
Concurrent hypokalemia worsens alkalosis through intracellular K⁺/H⁺ exchange and increased ammoniagenesis.
🔹
Unlike contraction alkalosis from diuretics, the alkalosis in primary hyperaldosteronism occurs despite volume expansion.
🔹
Board distinction: Volume-expanded alkalosis with hypokalemia → primary hyperaldosteronism; volume-contracted alkalosis with hypokalemia → diuretics or vomiting.

Cardiovascular Complications
⭐
Hyperaldosteronism causes cardiovascular damage beyond blood pressure effects alone through direct mineralocorticoid receptor activation.
⭐
Myocardial fibrosis, left ventricular hypertrophy, diastolic dysfunction, and increased arrhythmia risk (especially with hypokalemia).
⭐
Endothelial dysfunction, increased oxidative stress, and inflammation → accelerated atherosclerosis.
⭐
Higher rates of stroke, MI, and atrial fibrillation compared to essential hypertension matched for BP.
⭐
These effects are largely reversible with mineralocorticoid receptor blockade or surgical cure.
⭐
Board pearl: Cardiovascular risk in primary hyperaldosteronism exceeds that predicted by hypertension severity alone.

Differential Diagnosis: Mimics and Pitfalls
✅
Apparent mineralocorticoid excess: 11β-hydroxysteroid dehydrogenase deficiency → cortisol activates mineralocorticoid receptor. Caused by licorice (glycyrrhizin) or genetic defect.
✅
Liddle syndrome: gain-of-function ENaC mutation → constitutive Na⁺ reabsorption. Low renin, low aldosterone, responds to amiloride not spironolactone.
✅
Cushing syndrome: cortisol excess can overwhelm 11β-HSD2 → mineralocorticoid effects. Look for cushingoid features.
✅
Gordon syndrome (pseudohypoaldosteronism type II): WNK kinase mutations → increased NaCl reabsorption. Hyperkalemia despite hypertension.
✅
Board distinction: Hypertension with hypokalemia and LOW aldosterone → consider non-aldosterone mineralocorticoid excess.

Special Populations: Pregnancy and CKD
🧠
Pregnancy: physiologic RAAS activation makes diagnosis challenging. Aldosterone rises 5–10 fold but remains appropriate for pregnancy.
🧠
Spironolactone contraindicated in pregnancy (antiandrogen effects); use alternative agents like methyldopa, labetalol, or nifedipine.
🧠
CKD: hyperaldosteronism accelerates CKD progression through glomerular hyperfiltration, proteinuria, and tubulointerstitial fibrosis.
🧠
MR antagonists beneficial in CKD but increase hyperkalemia risk — start low dose with close monitoring.
🧠
Board pearl: Primary hyperaldosteronism is both a cause and consequence of CKD — screen CKD patients with resistant hypertension.

Monitoring and Follow-up
⚡
Post-surgical: monitor BP, K⁺, and creatinine. Expect transient hyperkalemia. Assess cure with repeat ARR after 3–6 months.
⚡
Medical therapy: check K⁺ and creatinine 1 week after initiation and dose changes, then every 3–6 months.
⚡
Titrate MR antagonist dose to normalize K⁺ (not just BP) — persistent hypokalemia indicates inadequate blockade.
⚡
Annual screening for target organ damage: echocardiogram for LVH, urine albumin for proteinuria.
⚡
Board pearl: Normalization of potassium is the best biochemical marker of adequate mineralocorticoid blockade.

Resistant Hypertension Workup
📌
Definition: BP above goal despite ≥3 antihypertensives including a diuretic, or controlled BP requiring ≥4 medications.
📌
Primary hyperaldosteronism is the most common secondary cause (20% of resistant hypertension).
📌
Other considerations: medication non-adherence, white coat effect, improper BP measurement, volume overload.
📌
Secondary cause workup: ARR for hyperaldosteronism, sleep study for OSA, renal artery imaging for RAS, 24h urine metanephrines for pheo.
📌
Board pearl: Every patient with resistant hypertension should be screened for primary hyperaldosteronism with ARR.

Board Question Stem Patterns
📣
Young patient + severe HTN + spontaneous hypokalemia → aldosterone-producing adenoma until proven otherwise.
📣
HTN + hypokalemia + metabolic alkalosis + low renin → primary hyperaldosteronism.
📣
HTN + hypokalemia + metabolic alkalosis + high renin → secondary hyperaldosteronism (RAS, diuretics, renin tumor).
📣
Resistant HTN on 3+ drugs including diuretic → screen with aldosterone-renin ratio.
📣
Post-adrenalectomy hyperkalemia → expected finding from chronic K⁺ depletion reversal.
📣
HTN that improves with dexamethasone → glucocorticoid-remediable aldosteronism.
📣
HTN + hypokalemia + low aldosterone → apparent mineralocorticoid excess or Liddle syndrome.

One-Line Recap
🔸
Hyperaldosteronism presents as hypertension with hypokalemia and metabolic alkalosis, distinguished as primary (high aldosterone, low renin from autonomous adrenal production) versus secondary (high aldosterone, high renin from RAAS activation), diagnosed by aldosterone-renin ratio and salt suppression testing, with adenomas cured surgically while bilateral hyperplasia requires lifelong mineralocorticoid receptor blockade.

bottom of page