top of page

eduo
visual

Reproductive & Endocrine Systems
Hormone Fluctuations and Feedback Loops
Core Principle of Hormone Feedback Loops
🧷
Endocrine homeostasis depends on feedback loops where hormone levels regulate their own production through effects on upstream control centers.
🧷
Negative feedback is the predominant mechanism: rising hormone levels suppress further release by inhibiting hypothalamic releasing hormones and/or pituitary tropic hormones.
🧷
Positive feedback is rare in physiology but critical in specific contexts: the LH surge triggering ovulation and oxytocin during labor.
🧷
The hypothalamic-pituitary-target organ axis exemplifies this principle across multiple systems (thyroid, adrenal, gonadal).
🧷
Board pearl: When hormone levels are discordant (e.g., high TSH with low T4), the feedback loop is intact; when both move in the same direction, suspect primary gland dysfunction or resistance.

The Hypothalamic-Pituitary Axis Architecture
📍
The hypothalamus secretes releasing or inhibiting hormones into the hypophyseal portal system, which carries them directly to the anterior pituitary.
📍
Key releasing hormones: TRH → TSH, CRH → ACTH, GnRH → LH/FSH, GHRH → GH.
📍
Key inhibiting hormones: somatostatin inhibits GH/TSH, dopamine inhibits prolactin.
📍
The posterior pituitary releases ADH and oxytocin, which are synthesized in hypothalamic nuclei and transported via axons.
📍
Board pearl: Portal system anatomy explains why pituitary stalk lesions cause hyperprolactinemia — loss of tonic dopamine inhibition.

Thyroid Hormone Feedback Loop
🔹
TRH from hypothalamus → TSH from anterior pituitary → T4/T3 from thyroid → negative feedback on both TRH and TSH.
🔹
Free T4 and T3 (not total levels) mediate feedback since only unbound hormone is biologically active.
🔹
T4 is converted to active T3 in peripheral tissues by 5'-deiodinase; this conversion is decreased in critical illness ("sick euthyroid syndrome").
🔹
Primary hypothyroidism: ↓T4/T3, ↑↑TSH (loss of negative feedback).
🔹
Primary hyperthyroidism: ↑T4/T3, ↓↓TSH (excessive negative feedback).
🔹
Board distinction: Central hypothyroidism shows ↓T4 with inappropriately normal or low TSH — the feedback loop cannot compensate.

Cortisol and the HPA Axis
⭐
CRH from hypothalamus → ACTH from anterior pituitary → cortisol from zona fasciculata of adrenal cortex.
⭐
Cortisol exhibits both negative feedback (on CRH/ACTH) and a distinct circadian rhythm: peaks at 8 AM, nadir at midnight.
⭐
Stress overrides negative feedback, allowing cortisol to rise despite already elevated levels.
⭐
Primary adrenal insufficiency (Addison's): ↓cortisol, ↑↑ACTH (plus hyperpigmentation from ACTH's MSH activity).
⭐
Cushing syndrome: ↑cortisol with variable ACTH depending on source.
⭐
Board pearl: Loss of circadian rhythm (elevated midnight cortisol) is more sensitive for Cushing's than a single morning level.

Sex Hormones: The HPG Axis in Males
✅
GnRH (pulsatile) → LH/FSH → testosterone from Leydig cells (LH) and spermatogenesis via Sertoli cells (FSH).
✅
Testosterone feeds back to inhibit GnRH and LH; inhibin B from Sertoli cells selectively inhibits FSH.
✅
Primary hypogonadism: ↓testosterone, ↑↑LH/FSH (e.g., Klinefelter syndrome).
✅
Secondary hypogonadism: ↓testosterone, ↓ or normal LH/FSH (e.g., Kallmann syndrome, pituitary tumor).
✅
Board pearl: Exogenous testosterone suppresses LH/FSH → testicular atrophy and infertility, which is why hCG (LH analog) is used to maintain fertility.

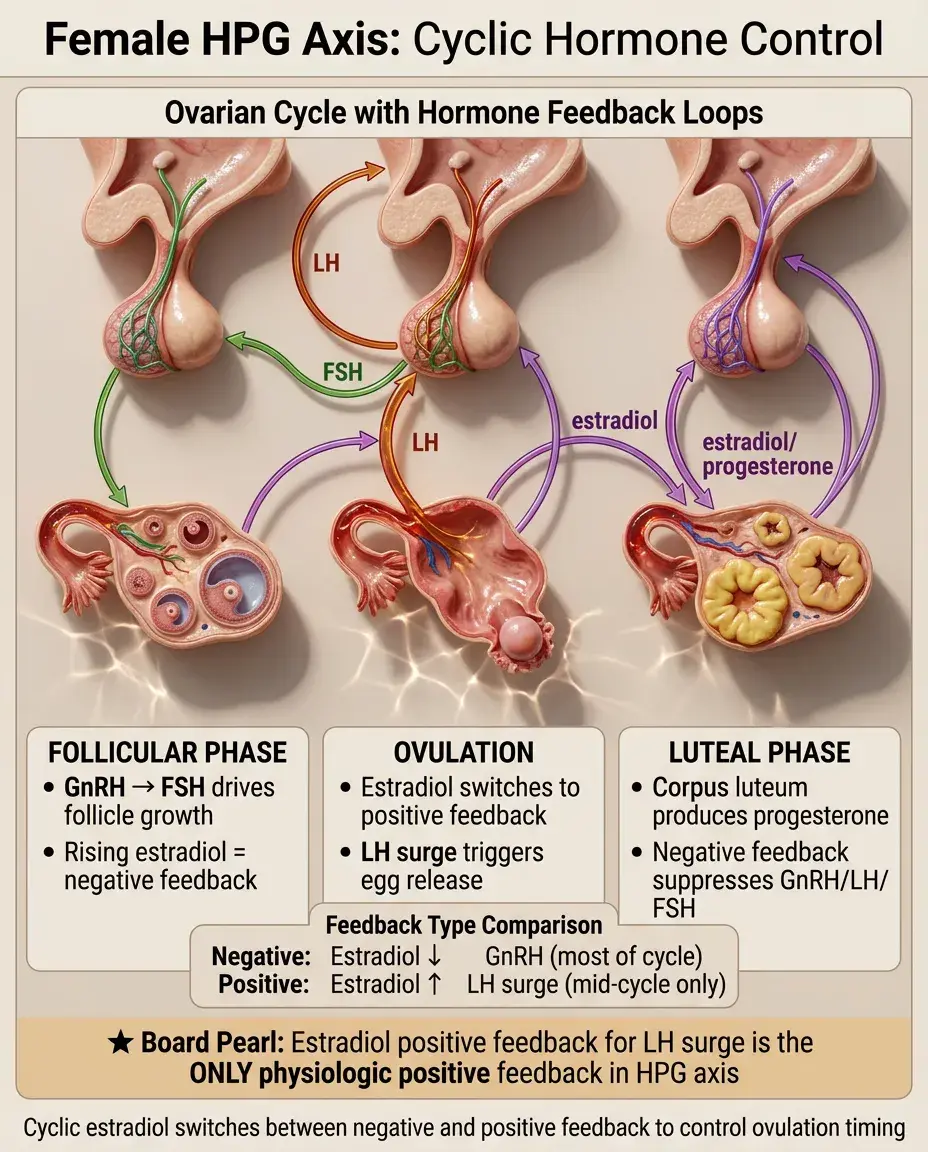
The Female HPG Axis: Cyclic Complexity
🧠
Follicular phase: GnRH → FSH → follicle growth and estradiol production → negative feedback keeps LH low.
🧠
Mid-cycle: rising estradiol switches from negative to positive feedback → LH surge → ovulation.
🧠
Luteal phase: corpus luteum produces progesterone and estradiol → negative feedback on GnRH/LH/FSH.
🧠
Without pregnancy, corpus luteum degenerates → hormone withdrawal → menstruation.
🧠
Board pearl: The estradiol positive feedback triggering the LH surge is the only physiologic positive feedback loop in the HPG axis.
Growth Hormone Regulation
⚡
GHRH stimulates and somatostatin inhibits GH release from somatotrophs.
⚡
GH acts directly and via IGF-1 (primarily from liver) to promote growth and metabolism.
⚡
IGF-1 mediates negative feedback on both GH and GHRH while stimulating somatostatin.
⚡
GH secretion is pulsatile with peaks during deep sleep, exercise, and hypoglycemia.
⚡
Acromegaly/gigantism: ↑GH, ↑IGF-1; GH deficiency: ↓GH, ↓IGF-1.
⚡
Board distinction: Random GH levels are unreliable due to pulsatility; IGF-1 reflects integrated GH secretion and is the preferred screening test.

Prolactin: The Exception to Negative Feedback
📌
Prolactin is unique: under tonic inhibition by dopamine from hypothalamus (not stimulated by a releasing hormone).
📌
Dopamine antagonists (antipsychotics), hypothyroidism (TRH stimulates prolactin), and pituitary stalk compression all cause hyperprolactinemia.
📌
Prolactin inhibits GnRH → hypogonadotropic hypogonadism → amenorrhea, infertility, decreased libido.
📌
During pregnancy/lactation, high prolactin is physiologic and maintains milk production.
📌
Board pearl: Mild prolactin elevation (< 100 ng/mL) suggests stalk effect or medication; very high levels (> 200 ng/mL) suggest prolactinoma.

Calcium Homeostasis and PTH Regulation
📣
Low ionized Ca²⁺ → PTH release → ↑Ca²⁺ via bone resorption, renal reabsorption, and 1,25(OH)₂D activation.
📣
High Ca²⁺ → suppresses PTH (negative feedback via calcium-sensing receptors on parathyroid cells).
📣
Primary hyperparathyroidism: ↑PTH, ↑Ca²⁺ (autonomous PTH secretion).
📣
Secondary hyperparathyroidism: ↑PTH, ↓ or normal Ca²⁺ (appropriate response to hypocalcemia, often from CKD or vitamin D deficiency).
📣
Board distinction: In hypercalcemia, PTH should be suppressed; detectable PTH suggests primary hyperparathyroidism.

Glucose Homeostasis: Insulin and Glucagon
🔸
Rising glucose → pancreatic β cells release insulin → glucose uptake and storage → glucose falls → insulin secretion stops.
🔸
Falling glucose → pancreatic α cells release glucagon → hepatic glucose production → glucose rises.
🔸
This is a rapid negative feedback system operating on a minute-to-minute basis.
🔸
Type 1 diabetes: loss of β cells → no insulin → no negative feedback on glucose.
🔸
Type 2 diabetes: insulin resistance → impaired negative feedback despite high insulin levels.
🔸
Board pearl: C-peptide distinguishes endogenous insulin (present) from exogenous insulin administration (C-peptide absent).

ADH and Water Balance
🧷
Hyperosmolality or hypovolemia → ADH release from posterior pituitary → water retention → dilutes plasma → ADH suppression.
🧷
ADH acts on V2 receptors in collecting duct → aquaporin-2 insertion → water reabsorption.
🧷
SIADH: inappropriate ADH despite low osmolality → hyponatremia with concentrated urine.
🧷
Central DI: absent ADH → dilute polyuria; nephrogenic DI: ADH resistance → same clinical picture.
🧷
Board pearl: Water deprivation test distinguishes DI types: central DI responds to desmopressin, nephrogenic does not.

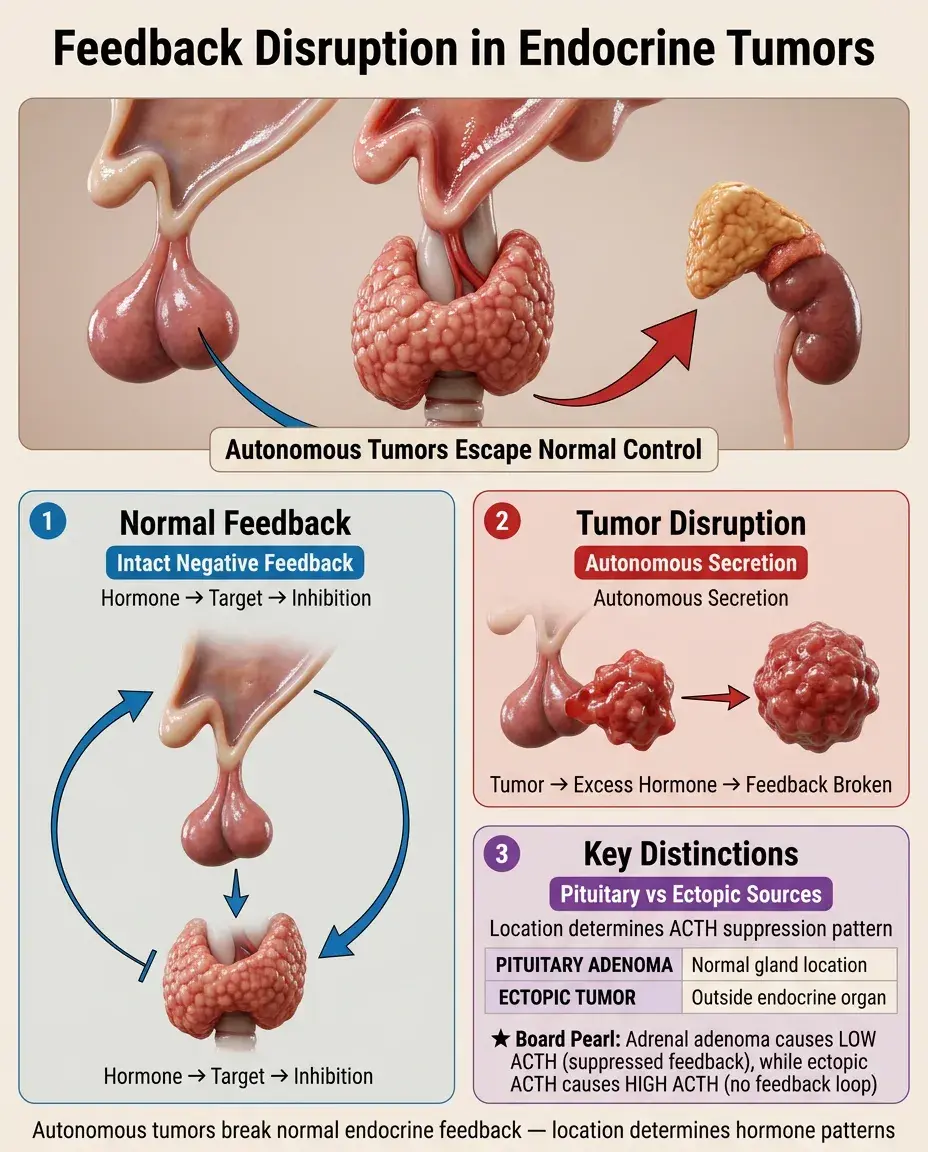
Feedback Disruption in Endocrine Tumors
📍
Autonomous hormone-secreting tumors escape normal feedback control.
📍
Pituitary adenomas: may secrete ACTH (Cushing disease), GH (acromegaly), or prolactin despite negative feedback.
📍
Adrenal adenomas: autonomous cortisol → suppressed ACTH (distinguishes from pituitary source).
📍
Thyroid adenomas: "hot nodules" produce T4/T3 independent of TSH.
📍
Board distinction: Ectopic hormone production (e.g., small cell lung cancer → ACTH) also escapes feedback but occurs outside the normal endocrine organ.
Dynamic Testing: Probing Feedback Integrity
🔹
Stimulation tests assess hormone reserve: ACTH stimulation for adrenal function, GnRH stimulation for gonadotropins.
🔹
Suppression tests identify autonomous secretion: dexamethasone for cortisol, glucose for GH.
🔹
Low-dose dexamethasone suppresses normal cortisol but not Cushing syndrome.
🔹
High-dose dexamethasone suppresses pituitary Cushing disease but not ectopic ACTH or adrenal adenoma.
🔹
Board pearl: The principle: normal glands respond to feedback manipulation, autonomous sources do not.

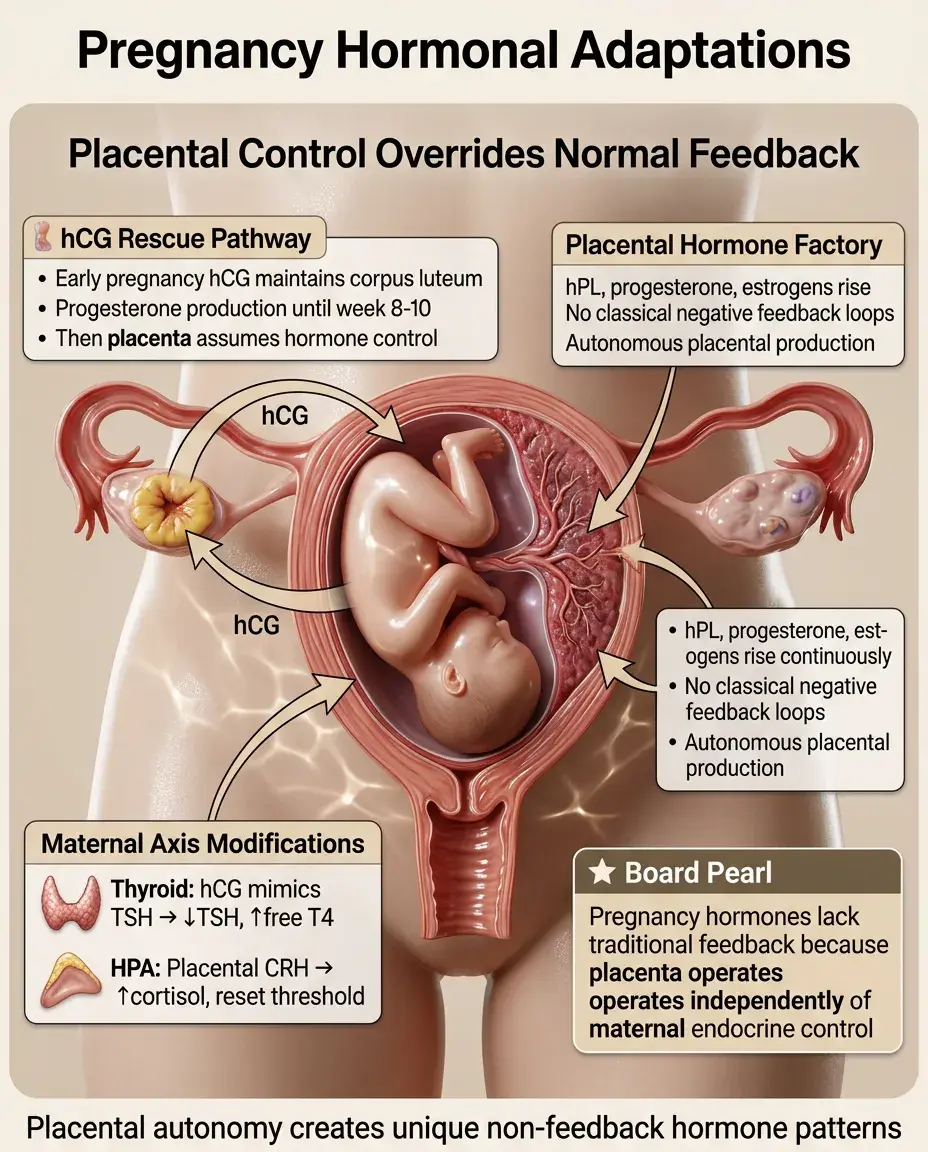
Pregnancy: Unique Hormonal Adaptations
⭐
hCG from trophoblast maintains corpus luteum → progesterone until placenta takes over (weeks 8-10).
⭐
Placental hormones (hPL, progesterone, estrogens) rise throughout pregnancy without classical feedback loops.
⭐
Maternal thyroid: hCG's TSH-like activity → mild TSH suppression and slight free T4 elevation in first trimester.
⭐
Maternal HPA axis: placental CRH → increased cortisol but reset feedback threshold.
⭐
Board pearl: Many pregnancy hormones lack traditional feedback because the placenta is not subject to maternal endocrine control.
Puberty: Reactivation of the HPG Axis
✅
During childhood, the HPG axis is actively suppressed despite capacity for function.
✅
Puberty begins with decreased hypothalamic sensitivity to negative feedback → increased GnRH pulsatility.
✅
Initial nocturnal LH pulses → gradual increase in sex steroids → secondary sexual characteristics.
✅
Adrenarche (DHEA-S rise) precedes gonadarche by ~2 years and is independent of HPG activation.
✅
Board distinction: Precocious puberty shows adult-pattern LH/FSH; premature adrenarche shows only elevated androgens.

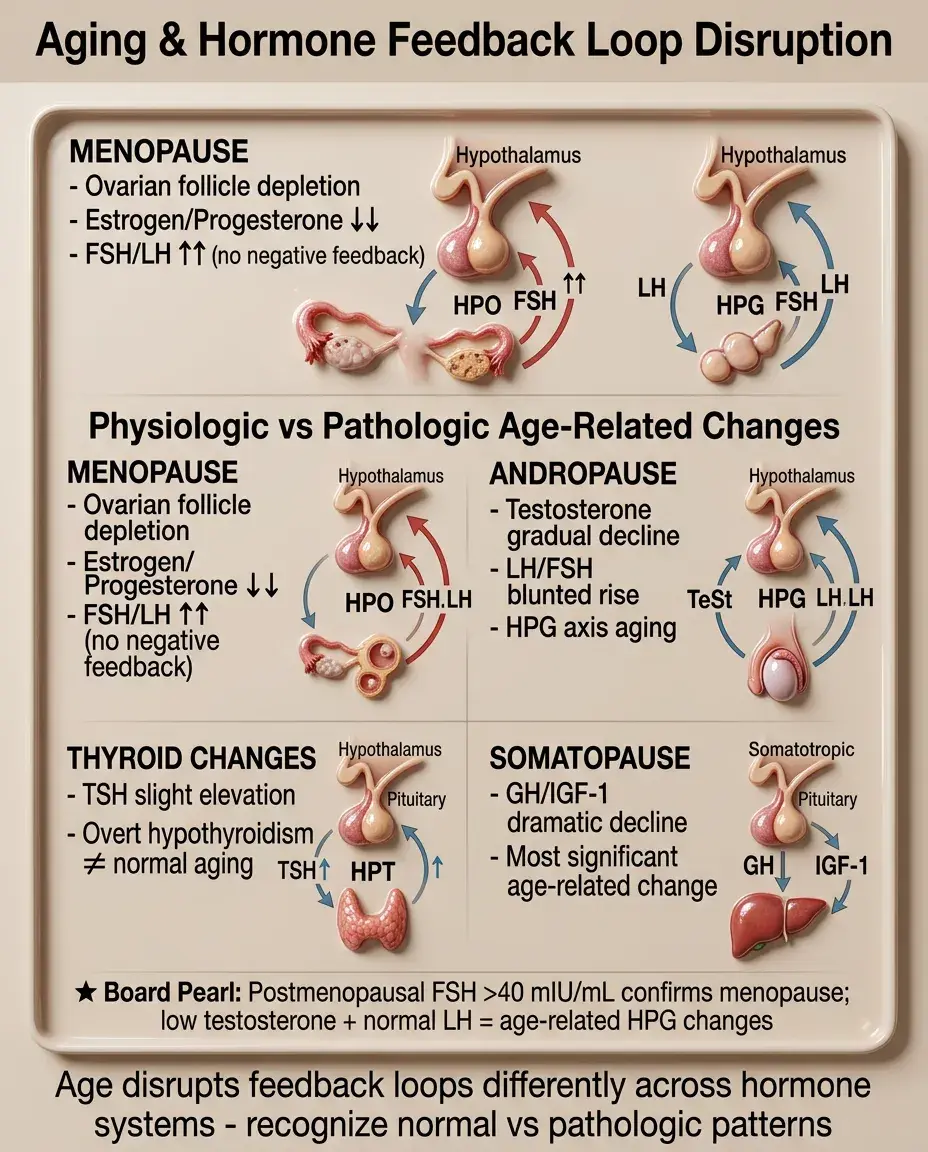
Aging and Feedback Loop Changes
🧠
Menopause: ovarian follicle depletion → loss of estrogen/progesterone → ↑↑FSH/LH (no negative feedback).
🧠
Andropause: gradual testosterone decline but LH/FSH rise is blunted (hypothalamic-pituitary aging).
🧠
Thyroid: TSH may rise slightly with age but overt hypothyroidism is not normal aging.
🧠
GH/IGF-1 axis shows the most dramatic decline: "somatopause."
🧠
Board pearl: Postmenopausal FSH > 40 mIU/mL confirms menopause; in men, low testosterone with normal LH suggests age-related HPG changes.
Stress and Override of Normal Feedback
⚡
Acute stress activates CRH/ACTH despite elevated cortisol — survival takes precedence over feedback.
⚡
Chronic stress can reset feedback sensitivity: persistent HPA activation despite high cortisol.
⚡
Critical illness suppresses TSH and gonadotropins ("sick euthyroid," hypogonadotropic hypogonadism) — adaptive response.
⚡
Hypoglycemia overrides normal GH suppression — glucose counterregulation is prioritized.
⚡
Board pearl: Stress-induced hormone changes are usually adaptive; treating the numbers without addressing the stressor is inappropriate.

Hormone Resistance Syndromes
📌
Resistance syndromes show high hormone levels with lack of appropriate tissue response.
📌
Androgen insensitivity: high testosterone, normal male karyotype, female phenotype.
📌
Thyroid hormone resistance: elevated T4/T3 with nonsuppressed TSH.
📌
Pseudohypoparathyroidism: high PTH with low calcium (PTH resistance).
📌
Type 2 diabetes: high insulin with hyperglycemia (insulin resistance).
📌
Board distinction: In resistance syndromes, feedback loops attempt to compensate by increasing hormone production, leading to characteristic lab patterns.

Board Question Stem Patterns
📣
High hormone with suppressed tropic hormone → primary hypersecretion or exogenous administration.
📣
Low hormone with elevated tropic hormone → primary gland failure with intact feedback.
📣
Both hormone and tropic hormone elevated → hormone resistance or ectopic production.
📣
Both hormone and tropic hormone low → secondary (central) deficiency.
📣
Normal hormone with very high tropic hormone → subclinical primary gland failure.
📣
Cyclical symptoms in a woman of reproductive age → consider menstrual cycle hormone fluctuations.
📣
Loss of circadian rhythm or stress response → suggests autonomous hormone production.

One-Line Recap
🔸
Hormone feedback loops maintain homeostasis through negative feedback where target hormones suppress their own production via hypothalamic-pituitary axes, with disruptions creating characteristic patterns — primary gland failure elevating tropic hormones, autonomous secretion suppressing them, and resistance syndromes showing inappropriate elevation of both — that guide diagnosis of endocrine disorders on board exams.

bottom of page