top of page

eduo
visual

Reproductive & Endocrine Systems
Follicular, Ovulatory, Luteal, and Menstrual Phases
Core Principle of the Menstrual Cycle
🧷
The menstrual cycle represents the coordinated interplay between the hypothalamic-pituitary-ovarian axis and the endometrium, preparing for potential pregnancy each month.
🧷
The cycle averages 28 days but can range from 21–35 days and consists of two parallel processes: the ovarian cycle (follicular → ovulation → luteal) and the uterine cycle (menstrual → proliferative → secretory).
🧷
GnRH from the hypothalamus drives pulsatile release of FSH and LH from the anterior pituitary, which act on the ovaries to produce estrogen and progesterone, which then feedback to regulate the HPO axis.
🧷
Board pearl: The follicular phase is variable in length, while the luteal phase is consistently 14 days.

Follicular Phase: Days 1–14
📍
Begins with menstruation (day 1) and ends with ovulation. Multiple primordial follicles are recruited by rising FSH, but only one becomes the dominant Graafian follicle.
📍
Granulosa cells have FSH receptors and produce estrogen via aromatization of androgens supplied by theca cells (two-cell theory).
📍
Rising estrogen levels cause negative feedback on FSH, allowing only the most FSH-sensitive follicle to survive while others undergo atresia.
📍
The endometrium is in the proliferative phase: estrogen stimulates endometrial thickening, straight glands, and spiral artery growth.
📍
Board pearl: FSH is highest in early follicular phase; estrogen rises throughout and peaks just before ovulation.

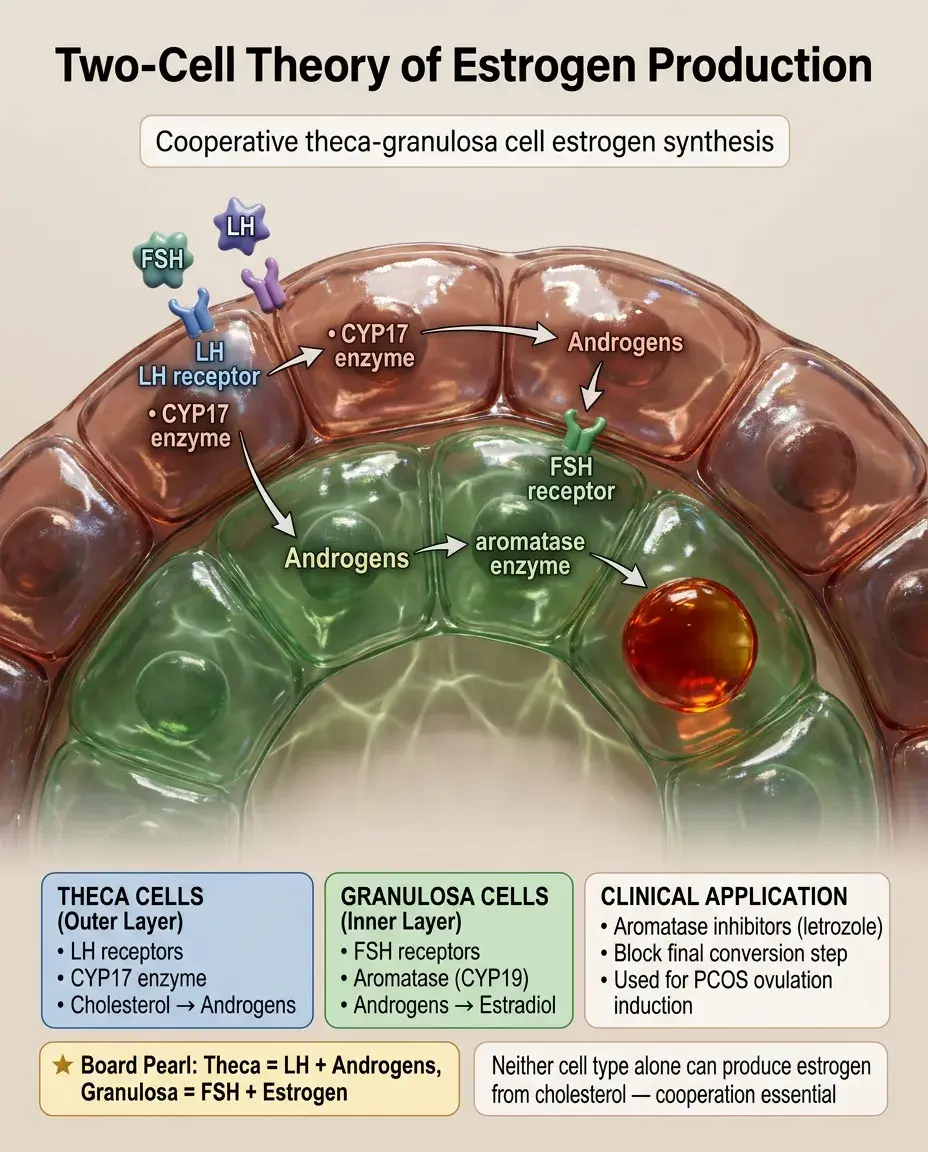
The Two-Cell Theory of Estrogen Production
🔹
Theca cells (LH receptors) convert cholesterol → androstenedione and testosterone using CYP17 (17α-hydroxylase).
🔹
These androgens diffuse to granulosa cells (FSH receptors), which use aromatase (CYP19) to convert androgens → estradiol.
🔹
This cooperation requires both cell types and both gonadotropins — neither cell type alone can produce estrogen from cholesterol.
🔹
Board distinction: Theca cells have LH receptors and make androgens; granulosa cells have FSH receptors and make estrogen.
🔹
Aromatase inhibitors (letrozole) block this final conversion step and are used for ovulation induction in PCOS.
The LH Surge and Ovulation: Day 14
⭐
When estrogen reaches a critical threshold (~200 pg/mL) for 36–48 hours, it switches from negative to positive feedback at the hypothalamus and pituitary.
⭐
This triggers a massive LH surge (and smaller FSH surge), occurring approximately 24–36 hours before ovulation.
⭐
The LH surge causes: completion of meiosis I (primary → secondary oocyte), breakdown of the follicle wall, and release of the cumulus-oocyte complex.
⭐
Ovulation typically occurs on day 14 of a 28-day cycle, releasing the oocyte into the peritoneal cavity where fimbriae guide it into the fallopian tube.
⭐
Board pearl: LH surge is what OPKs (ovulation predictor kits) detect; ovulation follows 24–36 hours later.

Luteal Phase: Days 15–28
✅
After ovulation, the remnant follicle transforms into the corpus luteum under continued LH stimulation.
✅
The corpus luteum produces high levels of progesterone and moderate estrogen, preparing the endometrium for implantation.
✅
Progesterone causes the endometrium to enter the secretory phase: glands become tortuous and secrete glycogen-rich fluid, spiral arteries coil, and stromal cells decidualize.
✅
Without pregnancy (no hCG), the corpus luteum degenerates after 14 days → corpus albicans, causing progesterone withdrawal.
✅
Board pearl: The luteal phase is always 14 days; variation in cycle length comes from the follicular phase.

Endometrial Changes Throughout the Cycle
🧠
Menstrual phase (days 1–5): progesterone withdrawal → spiral artery vasoconstriction → endometrial ischemia and shedding of the functional layer.
🧠
Proliferative phase (days 5–14): estrogen from growing follicles → endometrial regeneration, straight glands, increased thickness from 2–3 mm to 8–10 mm.
🧠
Secretory phase (days 15–28): progesterone from corpus luteum → glandular secretion, spiral artery coiling, stromal edema, preparation for implantation.
🧠
Board pearl: Endometrial dating: straight glands = proliferative (estrogen effect); coiled glands with secretions = secretory (progesterone effect).

Hormonal Feedback Mechanisms
⚡
Early follicular phase: low estrogen and progesterone → reduced negative feedback → rising GnRH, FSH, and LH.
⚡
Mid-follicular phase: rising estrogen from dominant follicle → negative feedback → declining FSH (prevents multiple ovulations).
⚡
Pre-ovulatory: sustained high estrogen → positive feedback → LH surge → ovulation.
⚡
Luteal phase: high progesterone + moderate estrogen → negative feedback → suppressed GnRH/FSH/LH.
⚡
Board pearl: Estrogen alone = negative feedback except when sustained at high levels (positive feedback for LH surge).

The Menstrual Phase: Days 1–5
📌
Triggered by corpus luteum degeneration → progesterone withdrawal → prostaglandin release (PGF2α) → spiral artery vasoconstriction.
📌
The functional layer (upper 2/3) of endometrium undergoes ischemic necrosis and is shed; the basal layer (lower 1/3) remains intact for regeneration.
📌
Normal menstrual flow: 30–40 mL blood loss over 3–7 days. >80 mL = menorrhagia.
📌
Prostaglandins cause myometrial contractions (cramping) and systemic effects (nausea, diarrhea).
📌
Board pearl: NSAIDs reduce menstrual flow and cramping by inhibiting prostaglandin synthesis.

Cervical Mucus Changes
📣
Follicular phase (low estrogen): thick, acidic mucus forms a plug preventing sperm entry.
📣
Periovulatory (high estrogen): thin, clear, alkaline, stretchy mucus (spinnbarkeit) with ferning pattern on microscopy — facilitates sperm transport.
📣
Luteal phase (progesterone): thick, opaque mucus returns, forming a protective barrier.
📣
Board pearl: Clear, stretchy cervical mucus indicates high estrogen/impending ovulation; thick mucus indicates progesterone dominance.
📣
Ferning pattern: estrogen effect causes crystallization of cervical mucus sodium chloride when dried on a slide.

Temperature Changes and the Biphasic Pattern
🔸
Basal body temperature (BBT) shows a biphasic pattern in ovulatory cycles.
🔸
Follicular phase: lower temperature (~97.0–97.5°F) due to estrogen's slight hypothermic effect.
🔸
Post-ovulation: temperature rises 0.5–1.0°F due to progesterone's thermogenic effect on the hypothalamus.
🔸
Temperature remains elevated throughout the luteal phase, dropping only with menstruation.
🔸
Board pearl: Sustained temperature elevation >16 days suggests pregnancy; monophasic BBT chart indicates anovulation.

Mittelschmerz and Ovulation Signs
🧷
Mittelschmerz: unilateral lower abdominal pain occurring at ovulation in ~20% of women, caused by follicular fluid irritating the peritoneum.
🧷
The pain typically lasts hours to 1–2 days and may alternate sides month to month.
🧷
Other ovulation signs: increased libido (testosterone peak), breast tenderness, clear cervical mucus, positive OPK.
🧷
Small amount of spotting may occur due to the brief estrogen drop immediately after ovulation.
🧷
Board pearl: Mid-cycle unilateral pelvic pain with clear mucus = mittelschmerz, a normal ovulation phenomenon.

Anovulatory Cycles
📍
Cycles without ovulation lack progesterone production, resulting in unopposed estrogen stimulation of the endometrium.
📍
Common at extremes of reproductive life (post-menarche, perimenopause) and with PCOS, hypothalamic dysfunction, hyperprolactinemia.
📍
Without progesterone withdrawal, bleeding occurs from unstable endometrium when estrogen levels fluctuate — often irregular and heavy.
📍
Long-term unopposed estrogen increases risk of endometrial hyperplasia and carcinoma.
📍
Board pearl: Irregular cycles with varying flow = likely anovulatory; regular cycles with consistent flow = likely ovulatory.

The Role of Inhibins
🔹
Inhibin B: produced by granulosa cells of growing follicles during the follicular phase; selectively inhibits FSH without affecting LH.
🔹
Inhibin A: produced by the corpus luteum during the luteal phase; continues selective FSH suppression.
🔹
These peptide hormones fine-tune the HPO axis by providing additional negative feedback specifically on FSH.
🔹
Activin (opposite effect) stimulates FSH release, but inhibins typically dominate.
🔹
Board pearl: Inhibin B = follicular phase marker; Inhibin A = luteal phase marker; both specifically suppress FSH.

The Fertile Window
⭐
The fertile window spans approximately 6 days: 5 days before ovulation plus ovulation day.
⭐
Sperm can survive up to 5 days in favorable cervical mucus; the oocyte survives only 12–24 hours after ovulation.
⭐
Peak fertility occurs on the day of the LH surge and the following day (day before and day of ovulation).
⭐
Timing intercourse to the fertile window is the basis of both natural family planning and fertility optimization.
⭐
Board pearl: Maximum conception probability occurs with intercourse 1–2 days before ovulation, not on ovulation day itself.

Luteal Phase Defect
✅
Inadequate progesterone production by the corpus luteum, resulting in a shortened luteal phase (<11 days) or insufficient endometrial development.
✅
Causes include subtle HPO axis dysfunction, thyroid disease, hyperprolactinemia, extreme exercise, low body weight.
✅
Presents as infertility or recurrent early pregnancy loss due to inadequate endometrial support.
✅
Diagnosis: mid-luteal progesterone <10 ng/mL or endometrial biopsy showing histologic lag.
✅
Board pearl: Short cycles (<21 days) often indicate luteal phase defect due to premature corpus luteum failure.

The Endometrial Window of Implantation
🧠
The endometrium is receptive to implantation only during a brief window: days 20–24 of a 28-day cycle (6–10 days post-ovulation).
🧠
Progesterone induces expression of integrins, pinopodes, and other adhesion molecules on the endometrial surface.
🧠
The blastocyst must hatch from the zona pellucida and appose, adhere, then invade the endometrium during this window.
🧠
Outside this window, the endometrium is refractory to implantation — a natural mechanism preventing ectopic timing.
🧠
Board pearl: Implantation occurs 6–10 days after fertilization, corresponding to days 20–24 of the cycle.

Hormonal Contraception and Cycle Suppression
⚡
Combined oral contraceptives provide constant levels of synthetic estrogen + progestin, suppressing GnRH pulsatility → no FSH/LH surge → no follicle development or ovulation.
⚡
The progestin component also thickens cervical mucus and causes endometrial atrophy, providing backup contraception.
⚡
Withdrawal bleeding during the placebo week mimics menstruation but represents artificial hormone withdrawal, not true endometrial cycling.
⚡
Continuous dosing (skipping placebos) safely suppresses withdrawal bleeding for extended periods.
⚡
Board pearl: OCPs prevent pregnancy primarily by inhibiting ovulation through HPO axis suppression.

Clinical Correlations and Pathology
📌
Oligomenorrhea (cycles >35 days): often anovulatory, associated with PCOS, thyroid disease, hyperprolactinemia.
📌
Polymenorrhea (cycles <21 days): suggests luteal phase defect or anovulation with frequent estrogen breakthrough.
📌
Amenorrhea workup: pregnancy test → TSH/prolactin → FSH (high = ovarian failure, low = hypothalamic/pituitary).
📌
Dysfunctional uterine bleeding: abnormal bleeding without structural cause, usually from anovulation and unopposed estrogen.
📌
Board pearl: First-line treatment for anovulatory bleeding is progestins to oppose estrogen and trigger organized withdrawal bleed.

Board Question Stem Patterns
📣
Woman with regular 28-day cycles has unilateral pelvic pain on cycle day 14 → mittelschmerz from ovulation.
📣
Clear, stretchy cervical mucus that forms fern pattern → periovulatory high estrogen state.
📣
Basal body temperature rises on day 15 and stays elevated → progesterone effect confirming ovulation.
📣
Endometrial biopsy shows straight glands and mitotic figures → proliferative phase (estrogen effect).
📣
Tortuous glands with glycogen-rich secretions → secretory phase (progesterone effect).
📣
Cycles varying from 24–65 days with heavy flow → anovulatory cycles with unopposed estrogen.
📣
Mid-luteal progesterone of 2 ng/mL → anovulation (ovulatory cycles show >10 ng/mL).

One-Line Recap
🔸
The menstrual cycle coordinates follicular development (FSH → estrogen), ovulation (LH surge), and luteal function (progesterone) with corresponding endometrial changes (menstrual shedding → proliferative growth → secretory preparation), creating a precise 28-day system where the variable follicular phase determines cycle length while the luteal phase remains fixed at 14 days.

bottom of page