top of page

eduo
visual

Biostatistics & Epidemiology
Determinants of Healthcare Utilization
Core Principle of Healthcare Utilization
🧷
Healthcare utilization refers to the frequency and pattern with which individuals access health services — from preventive care to emergency department visits to specialty consultations.
🧷
Utilization is determined by a complex interplay of factors: patient need, ability to access care, predisposing characteristics, and health system factors.
🧷
The Andersen Behavioral Model provides the foundational framework: Predisposing factors → Enabling factors → Need factors → Healthcare use.
🧷
Understanding these determinants helps explain disparities in healthcare access and outcomes across different populations.
🧷
Board pearl: Questions often present scenarios where multiple factors interact — identify the primary barrier limiting utilization.

Predisposing Factors: Demographics and Beliefs
📍
Predisposing factors are individual characteristics that exist prior to illness and influence the likelihood of seeking care.
📍
Demographics: age (very young and elderly use more), gender (women use more preventive services), education level (higher education → more preventive care use).
📍
Health beliefs and attitudes: perceived susceptibility to illness, perceived benefits of treatment, cultural beliefs about medicine, past healthcare experiences.
📍
Social structure: occupation, social networks, family size — all influence healthcare-seeking behavior.
📍
Board distinction: Predisposing factors influence the propensity to use services but don't guarantee access.

Enabling Factors: Resources and Access
🔹
Enabling factors are the resources that facilitate or impede healthcare use — they turn predisposition into action.
🔹
Personal enabling resources: income, health insurance status, having a regular source of care, transportation, ability to take time off work.
🔹
Community enabling resources: availability of providers, geographic proximity to care, appointment availability, public transportation.
🔹
Board pearl: Insurance is the single most important enabling factor in the US healthcare system — uninsured individuals use 50% less healthcare than insured.
🔹
Even with insurance, underinsurance (high deductibles, limited coverage) creates financial barriers to utilization.

Need Factors: Perceived and Evaluated Need
⭐
Need is the most immediate determinant of healthcare use — people must recognize a problem exists.
⭐
Perceived need: individual's own assessment of their health status and need for care. Influenced by symptom recognition, health literacy, and illness beliefs.
⭐
Evaluated need: professional judgment about health status and need for medical care. Often measured by diagnoses, symptom severity, and functional status.
⭐
Discordance between perceived and evaluated need explains many utilization patterns — patients may not recognize serious conditions or may seek care for minor self-limiting problems.
⭐
Board concept: Low health literacy → poor symptom recognition → delayed care seeking → worse outcomes.

Health Insurance as a Primary Determinant
✅
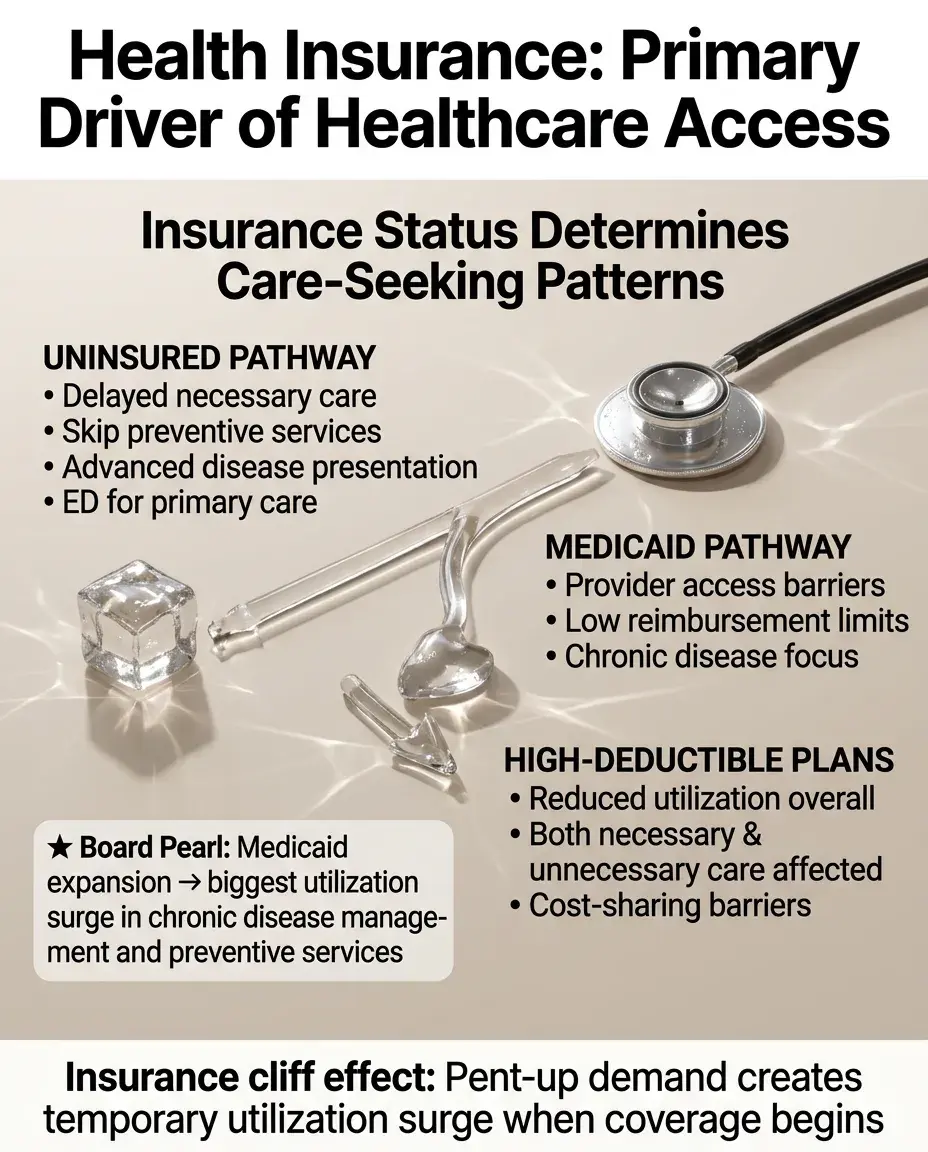
Insurance status is the strongest predictor of healthcare utilization in the United States.
✅
Uninsured individuals: delay necessary care, skip preventive services, present with more advanced disease, use emergency departments for primary care.
✅
Insurance type matters: Medicaid patients face provider access barriers due to low reimbursement rates; high-deductible plans reduce both necessary and unnecessary utilization.
✅
The "insurance cliff effect": gaining insurance leads to pent-up demand → temporary surge in utilization as previously unmet needs are addressed.
✅
Board pearl: When insurance expands (e.g., Medicaid expansion), utilization increases most for chronic disease management and preventive services.
Socioeconomic Status and Utilization Gradients
🧠
Lower SES → lower utilization of preventive services but higher emergency department use — the "inverse care law."
🧠
Income affects utilization through multiple pathways: ability to pay for care, time costs of seeking care, health literacy, neighborhood resources.
🧠
Education influences health literacy → symptom recognition → appropriate care seeking → navigation of complex health systems.
🧠
Wealth (assets) provides buffer for health shocks — those without savings delay care due to cost concerns.
🧠
Board distinction: SES affects not just whether people use care, but where they seek it (ED vs primary care) and when (crisis vs prevention).

Geographic and Spatial Determinants
⚡
Rural residents face unique barriers: provider shortages, long travel distances, limited specialty care, hospital closures.
⚡
Urban residents may face different barriers: transportation despite proximity, long wait times, fragmented care across multiple sites.
⚡
"Medical deserts": areas with inadequate healthcare infrastructure relative to population needs — common in rural areas and poor urban neighborhoods.
⚡
Spatial mismatch: healthcare facilities concentrated in affluent areas while need is greatest in underserved communities.
⚡
Board concept: Distance to care is measured not just in miles but in time and transportation costs — "effective distance.

Cultural and Linguistic Factors
📌
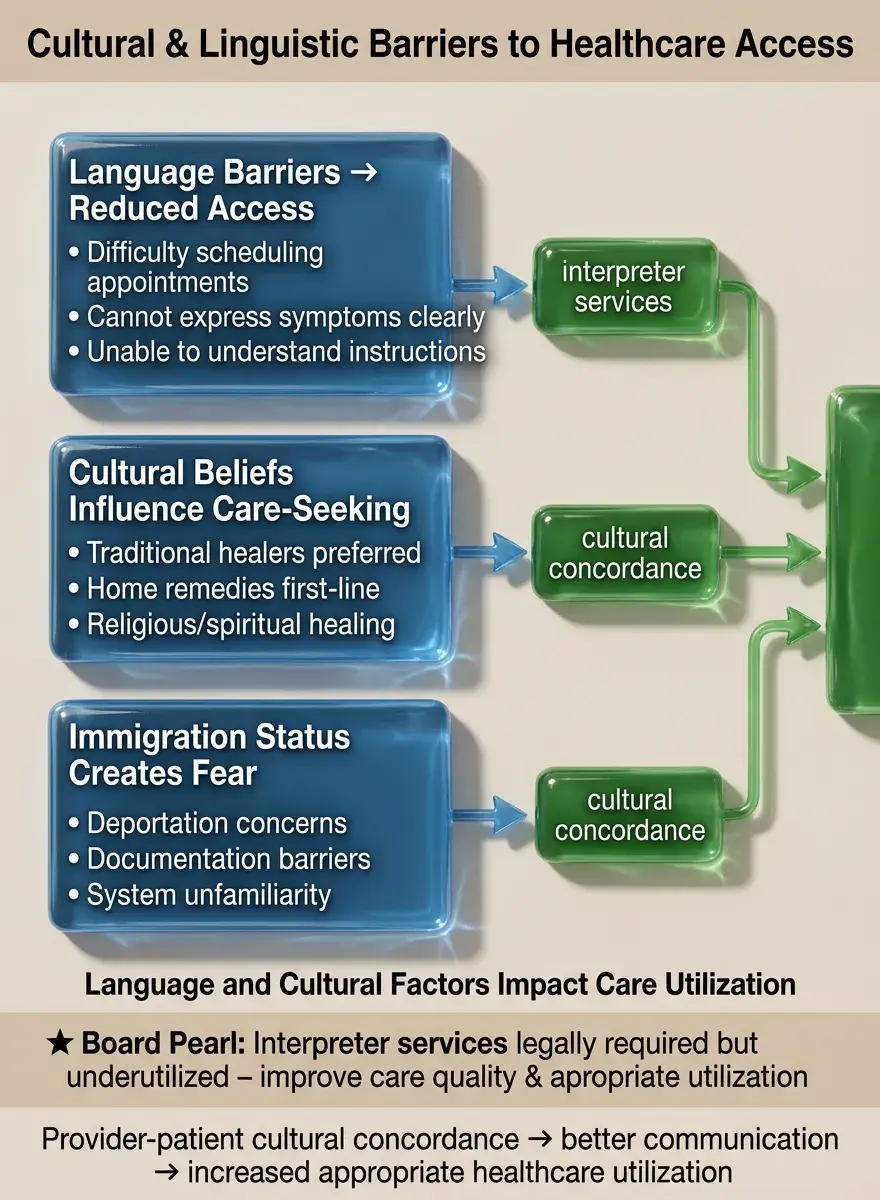
Language barriers reduce utilization: difficulty making appointments, understanding instructions, expressing symptoms, navigating systems.
📌
Cultural beliefs about illness causation and treatment influence when and where people seek care — traditional healers, home remedies, prayer.
📌
Provider-patient cultural concordance improves communication, trust, and adherence → increased appropriate utilization.
📌
Immigration status affects utilization through fear of deportation, lack of documentation for insurance, unfamiliarity with US healthcare system.
📌
Board pearl: Interpreter services are legally required but underutilized — their use improves care quality and appropriate utilization.
Health System Characteristics
📣
Provider availability: specialist shortages → long wait times → delayed care; primary care shortages → inappropriate ED use.
📣
Appointment systems: same-day availability increases utilization for acute needs; long waits decrease preventive care use.
📣
Care coordination: fragmented systems → duplicate tests, missed diagnoses, patient frustration → reduced engagement.
📣
Quality of care: past negative experiences → reduced future utilization; positive experiences → appropriate ongoing care.
📣
Board distinction: Supply-induced demand — more providers in an area can lead to higher utilization independent of need.

Psychological and Behavioral Factors
🔸
Depression reduces utilization for physical health needs — apathy, hopelessness, reduced self-care, social withdrawal.
🔸
Anxiety can both increase (health anxiety → frequent visits) and decrease (avoidance of feared diagnoses) utilization.
🔸
Substance use disorders: chaotic utilization patterns — missed appointments but frequent ED visits, poor preventive care.
🔸
Cognitive impairment: inability to recognize symptoms, remember appointments, navigate systems → underutilization until crisis.
🔸
Board concept: Mental health conditions create bidirectional effects — they affect physical health utilization and are themselves underdiagnosed due to stigma.

Age-Specific Utilization Patterns
🧷
Children: utilization driven by parents — parental education, anxiety, and experience shape pediatric healthcare use.
🧷
Adolescents: lowest utilization rates — transition from pediatric care, confidentiality concerns, sense of invulnerability.
🧷
Working-age adults: utilization constrained by time costs — difficulty taking time off work, competing responsibilities.
🧷
Elderly: highest utilization — multiple chronic conditions, Medicare coverage, but may underutilize due to transportation or cognitive barriers.
🧷
Board pearl: The "birthday effect" — utilization spikes at age 65 when Medicare eligibility begins, revealing previously unmet need.

Gender Differences in Healthcare Seeking
📍
Women utilize more healthcare services across the lifespan — reproductive health needs, greater preventive care use, different symptom perception.
📍
Men delay care seeking — social norms about masculinity, minimization of symptoms, preference for self-reliance.
📍
Gender-specific barriers: women face time constraints from caregiving roles; men face stigma for mental health care seeking.
📍
Transgender individuals face unique barriers: discrimination, lack of knowledgeable providers, insurance exclusions.
📍
Board distinction: Gender differences are most pronounced in preventive care and least pronounced in emergency care.

Race, Ethnicity, and Healthcare Disparities
🔹
Racial/ethnic minorities have lower utilization of preventive services and specialty care but higher ED use.
🔹
Historical mistrust of healthcare systems due to discrimination and unethical research reduces care seeking among minorities.
🔹
Provider bias affects referral patterns — minorities less likely to be referred for advanced procedures even with same clinical presentation.
🔹
Residential segregation concentrates minorities in areas with fewer healthcare resources.
🔹
Board pearl: Disparities persist even after controlling for insurance and income — suggesting discrimination and cultural factors play independent roles.

Social Support and Network Effects
⭐
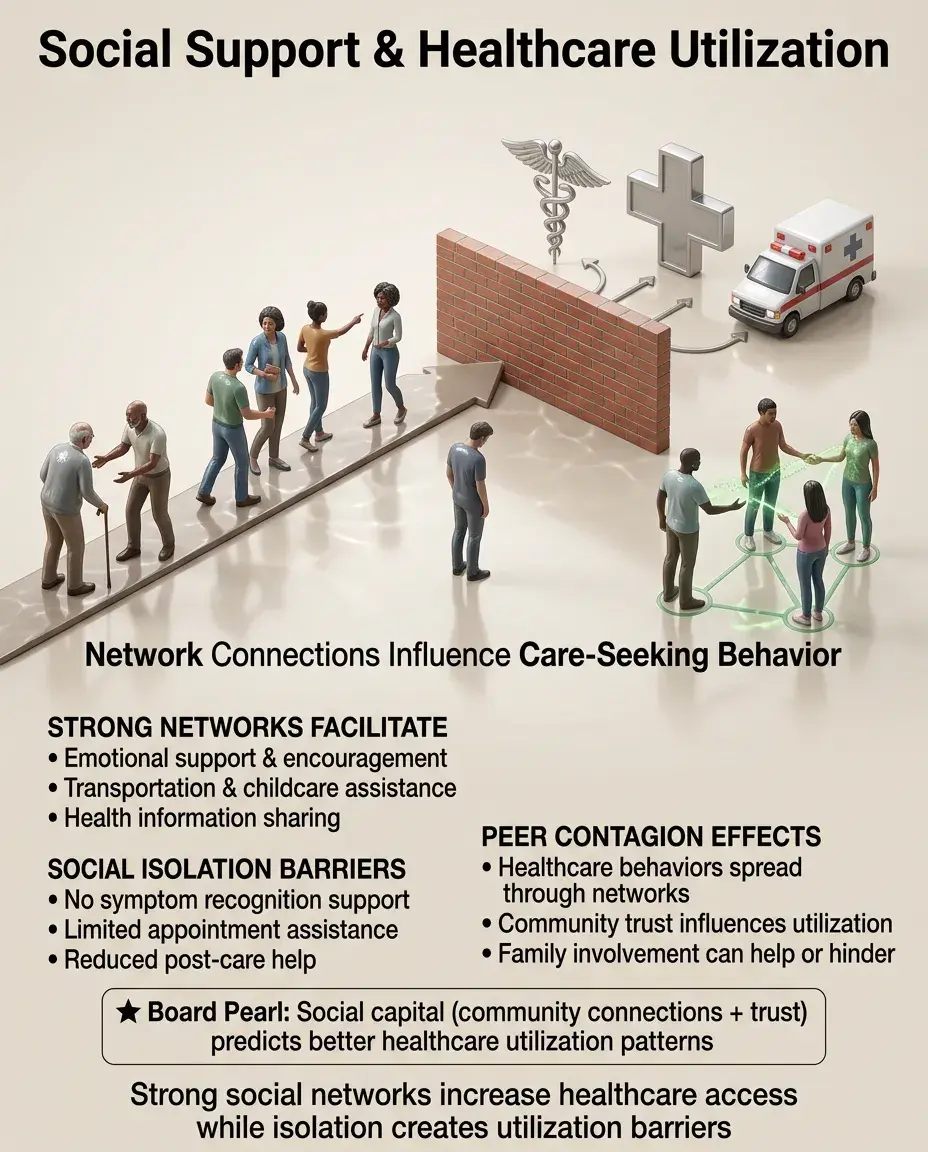
Strong social networks increase utilization through: emotional support, practical assistance (transportation, childcare), health information sharing.
⭐
Social isolation reduces utilization — no one to notice symptoms, assist with appointments, provide post-care support.
⭐
Family involvement can facilitate (encouragement to seek care) or hinder (conflicting advice, traditional healing preferences) utilization.
⭐
Peer effects: healthcare use by social network members influences individual behavior — "contagion" of health behaviors.
⭐
Board concept: Social capital — community connections and trust — predicts better healthcare utilization patterns.
Time Costs and Competing Priorities
✅
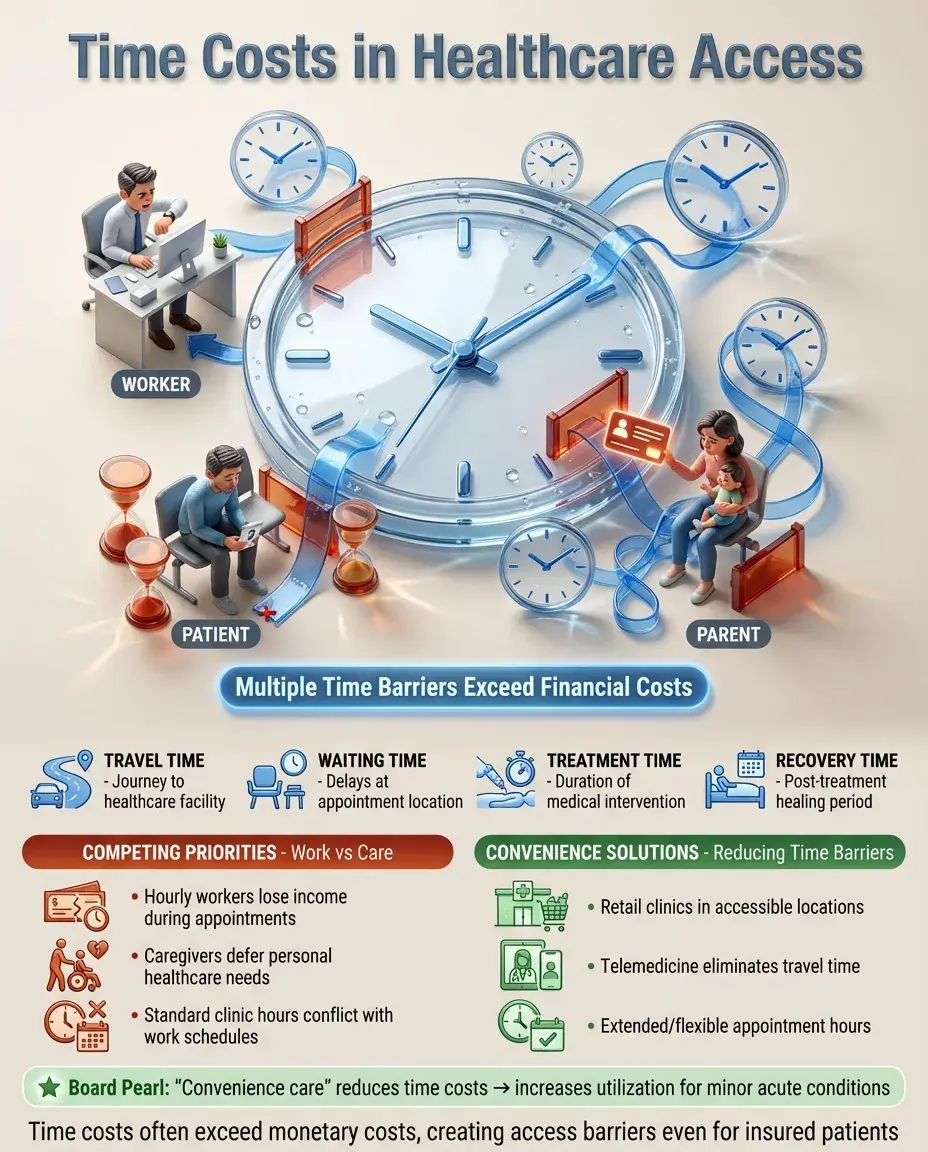
Time costs include: travel time, waiting time, treatment time, recovery time — often exceed monetary costs for low-income workers.
✅
Hourly workers face income loss for medical appointments → delay care until urgent → costlier interventions.
✅
Caregiving responsibilities compete with personal healthcare needs — parents and caregivers often defer their own care.
✅
Clinic hours that conflict with work schedules create access barriers even for insured patients.
✅
Board pearl: "Convenience care" (retail clinics, telemedicine) reduces time costs → increases utilization for minor acute conditions.
Health Literacy and Navigation Skills
🧠
Low health literacy → inability to recognize concerning symptoms → delayed presentation → worse outcomes.
🧠
System navigation skills: understanding insurance benefits, finding in-network providers, making appointments, following referrals.
🧠
Complex healthcare systems disadvantage those with limited education or cognitive resources.
🧠
Health literacy affects medication adherence, follow-up compliance, and appropriate use of emergency vs routine care.
🧠
Board distinction: Health literacy is distinct from general literacy — educated patients may still struggle with medical complexity.

Policy Interventions and Utilization Changes
⚡
Insurance expansions (ACA, Medicaid expansion) → increased utilization, especially preventive care and chronic disease management.
⚡
Cost-sharing (copays, deductibles) → reduces both necessary and unnecessary care — "blunt instrument" that doesn't discriminate.
⚡
Patient-centered medical homes → better care coordination → more appropriate utilization patterns.
⚡
Telemedicine expansion → reduces geographic and time barriers → increases access for rural and mobility-limited patients.
⚡
Board pearl: Value-based payment models aim to optimize utilization — incentivizing prevention and care coordination over volume.

Emergency Department Utilization Patterns
📌
ED use for non-urgent conditions reflects access barriers: lack of primary care, inability to get timely appointments, after-hours needs.
📌
Frequent ED users (≥4 visits/year) often have complex medical and social needs — chronic conditions, mental illness, substance use, homelessness.
📌
Insurance status paradox: Medicaid patients use ED more than uninsured due to access barriers to primary care despite coverage.
📌
EMTALA ensures emergency evaluation regardless of ability to pay → ED becomes "safety net of the safety net."
📌
Board concept: Reducing inappropriate ED use requires addressing upstream access barriers, not just educating patients.

Board Question Stem Patterns
📣
Uninsured patient delays seeking care for chest pain → presents with large MI → insurance as enabling factor.
📣
Rural patient unable to access specialist care → geographic barriers and provider availability.
📣
Non-English speaking patient misses follow-up appointments → language as cultural barrier.
📣
Elderly patient with multiple missed appointments after spouse dies → social support as enabling factor.
📣
Working mother skips mammogram due to clinic hours → time costs and competing priorities.
📣
Patient uses ED for prescription refill → primary care access barriers.
📣
Medicaid expansion leads to surge in diabetes diagnoses → pent-up demand and improved access.

One-Line Recap
🔸
Healthcare utilization is determined by the complex interaction of predisposing factors (demographics, beliefs), enabling factors (insurance, income, geographic access), and need factors (perceived and evaluated health status), with insurance status serving as the primary driver in the US system, creating predictable patterns where vulnerable populations paradoxically have both underutilization of preventive care and overutilization of emergency services.

bottom of page