top of page

eduo
visual

Biostatistics & Epidemiology
Community and Global Health Initiatives
Core Principle of Community and Global Health Initiatives
🧷
Community and global health initiatives focus on improving health outcomes at population levels through prevention, health promotion, and addressing social determinants of health.
🧷
Unlike individual clinical care, these initiatives target entire communities or populations using epidemiological data to identify health disparities and implement evidence-based interventions.
🧷
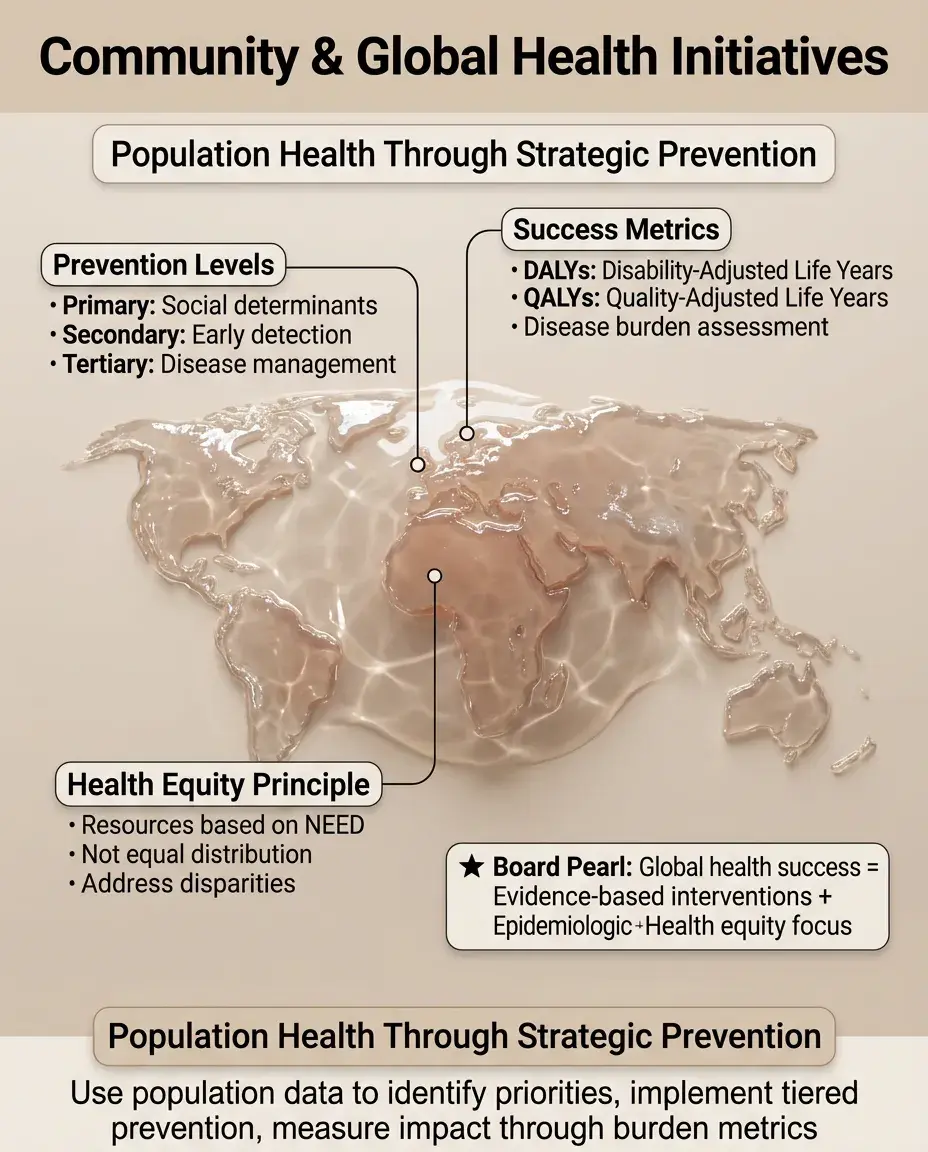
Success is measured by population health metrics: mortality rates, disease incidence, disability-adjusted life years (DALYs), and quality-adjusted life years (QALYs).
🧷
Board pearl: Questions often present scenarios requiring you to distinguish between individual-level interventions (clinical care) and population-level interventions (public health programs).

Primary, Secondary, and Tertiary Prevention Framework
📍
Primary prevention: preventing disease before it occurs through risk factor modification — vaccination programs, water sanitation, health education, policy interventions (seatbelt laws, tobacco taxes).
📍
Secondary prevention: early detection and treatment of disease to prevent progression — screening programs (mammography, colonoscopy), contact tracing for infectious diseases.
📍
Tertiary prevention: managing disease to slow or stop progression and prevent complications — cardiac rehabilitation, diabetes management programs.
📍
Board distinction: Vaccination is primary prevention; screening asymptomatic individuals is secondary prevention; treating established disease is tertiary prevention.

Social Determinants of Health
🔹
Social determinants account for 80% of health outcomes, far exceeding the impact of medical care (20%).
🔹
Key domains: economic stability (poverty, employment), education access, healthcare access, neighborhood environment (housing quality, crime, food deserts), social context (discrimination, social support).
🔹
Health disparities arise when social determinants create unequal opportunities for health across different populations.
🔹
Board pearl: When asked about the most effective intervention to improve population health, prioritize addressing social determinants over expanding clinical services.

Health Equity vs Health Equality
⭐
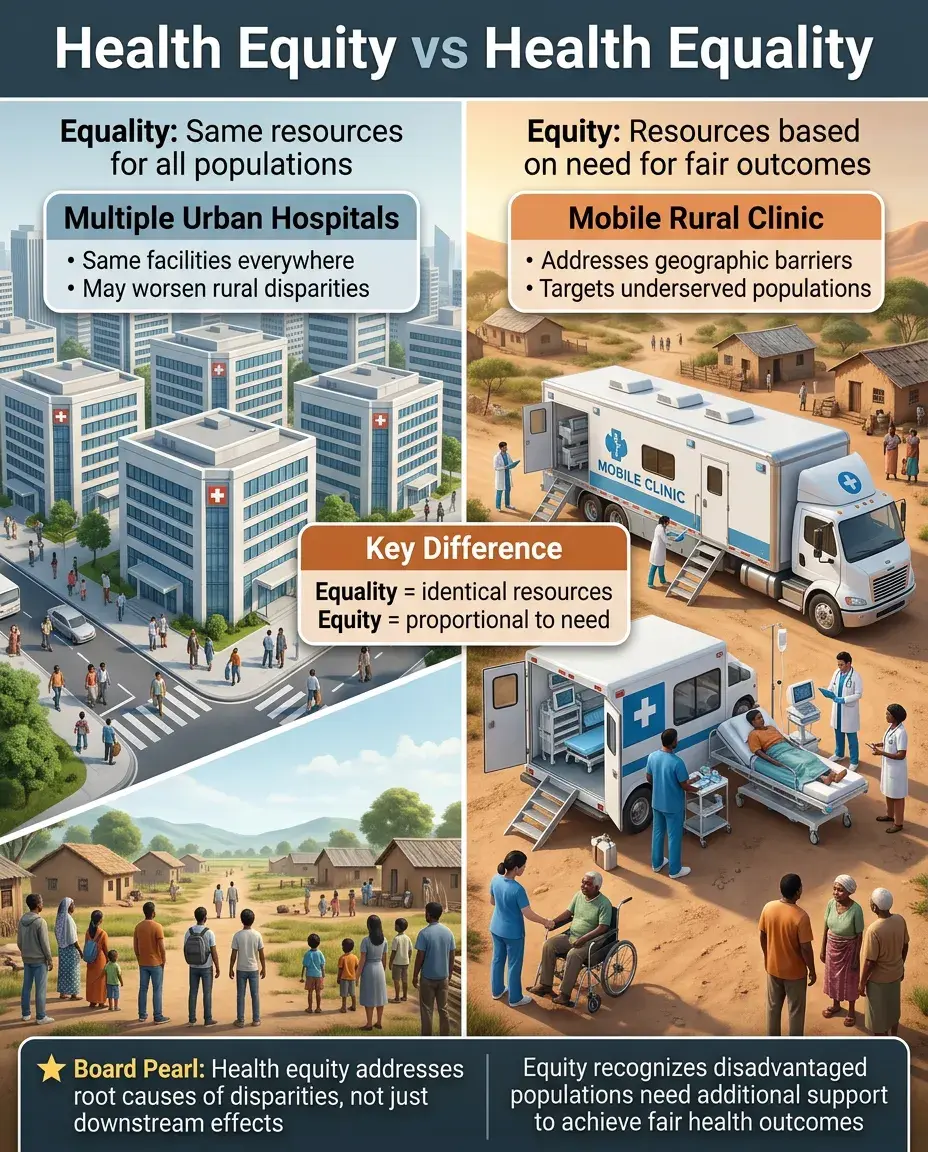
Health equality: providing the same resources and opportunities to all populations regardless of need.
⭐
Health equity: providing resources based on need to achieve fair outcomes — recognizing that disadvantaged populations require additional support to overcome barriers.
⭐
Achieving health equity requires identifying and addressing root causes of disparities, not just treating downstream effects.
⭐
Example: Mobile clinics in rural areas represent equity (addressing geographic barriers), while building more hospitals in cities represents equality but may worsen disparities.
Community Health Assessment and Planning
✅
Community health assessment involves systematic collection and analysis of health data to identify priority health problems and resources.
✅
Key steps: define community boundaries, collect quantitative data (vital statistics, disease surveillance) and qualitative data (focus groups, key informant interviews), identify health priorities, develop action plans.
✅
Data sources include vital statistics, disease registries, hospital discharge data, behavioral risk factor surveys, and census data.
✅
Board pearl: The most important first step in any community health initiative is conducting a needs assessment to understand the specific health challenges and assets of the target population.

Global Disease Burden Metrics
🧠
Disability-Adjusted Life Years (DALYs): sum of years of life lost (YLL) due to premature mortality and years lived with disability (YLD).
🧠
Quality-Adjusted Life Years (QALYs): measure of disease burden including both quality and quantity of life lived.
🧠
Global Burden of Disease Study tracks DALYs across countries to identify leading causes of death and disability worldwide.
🧠
Board distinction: DALYs measure disease burden (higher = worse); QALYs measure health benefit (higher = better). Cost-effectiveness analyses often use cost per QALY gained.

Infectious Disease Control in Global Health
⚡
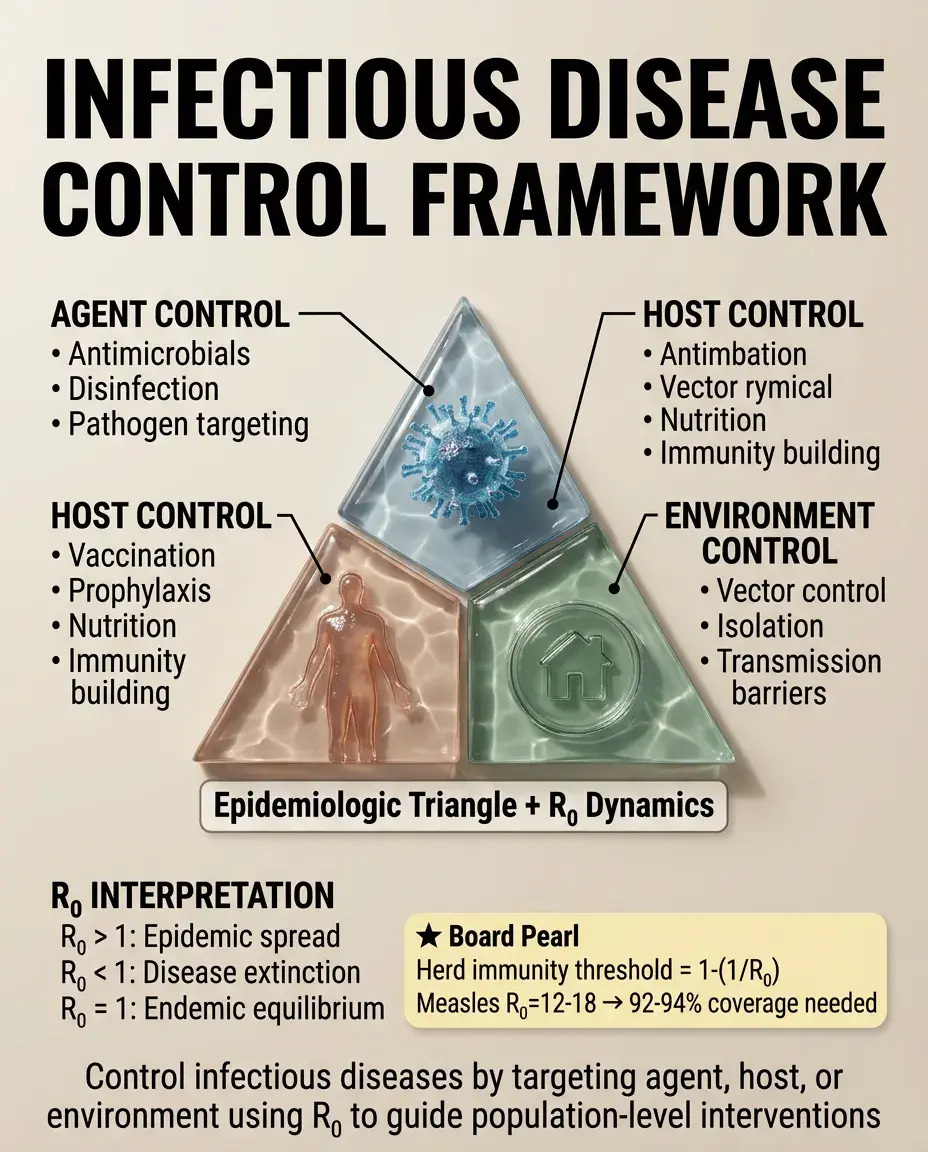
The epidemiologic triangle: agent (pathogen), host (susceptible individual), environment (conditions promoting transmission).
⚡
Control strategies target each component: agent (antimicrobials, disinfection), host (vaccination, prophylaxis, nutrition), environment (sanitation, vector control, isolation).
⚡
R₀ (basic reproduction number): average number of secondary cases from one infected individual in a susceptible population. R₀ > 1 means epidemic spread; R₀ < 1 means disease dies out.
⚡
Board pearl: Herd immunity threshold = 1 - (1/R₀). For measles with R₀ = 12-18, herd immunity requires 92-94% vaccination coverage.
Water, Sanitation, and Hygiene (WASH)
📌
WASH interventions have the highest impact on global disease burden, preventing diarrheal diseases, soil-transmitted helminths, schistosomiasis, and trachoma.
📌
Improved water sources: piped water, protected wells/springs, rainwater collection. Unimproved: surface water, unprotected wells.
📌
Improved sanitation: flush toilets, pit latrines with slabs. Unimproved: open defecation, shared facilities, pit latrines without slabs.
📌
Board clue: Diarrheal disease remains the second leading cause of death in children under 5 globally, with 88% attributable to unsafe water, inadequate sanitation, and poor hygiene.

Maternal and Child Health Initiatives
📣
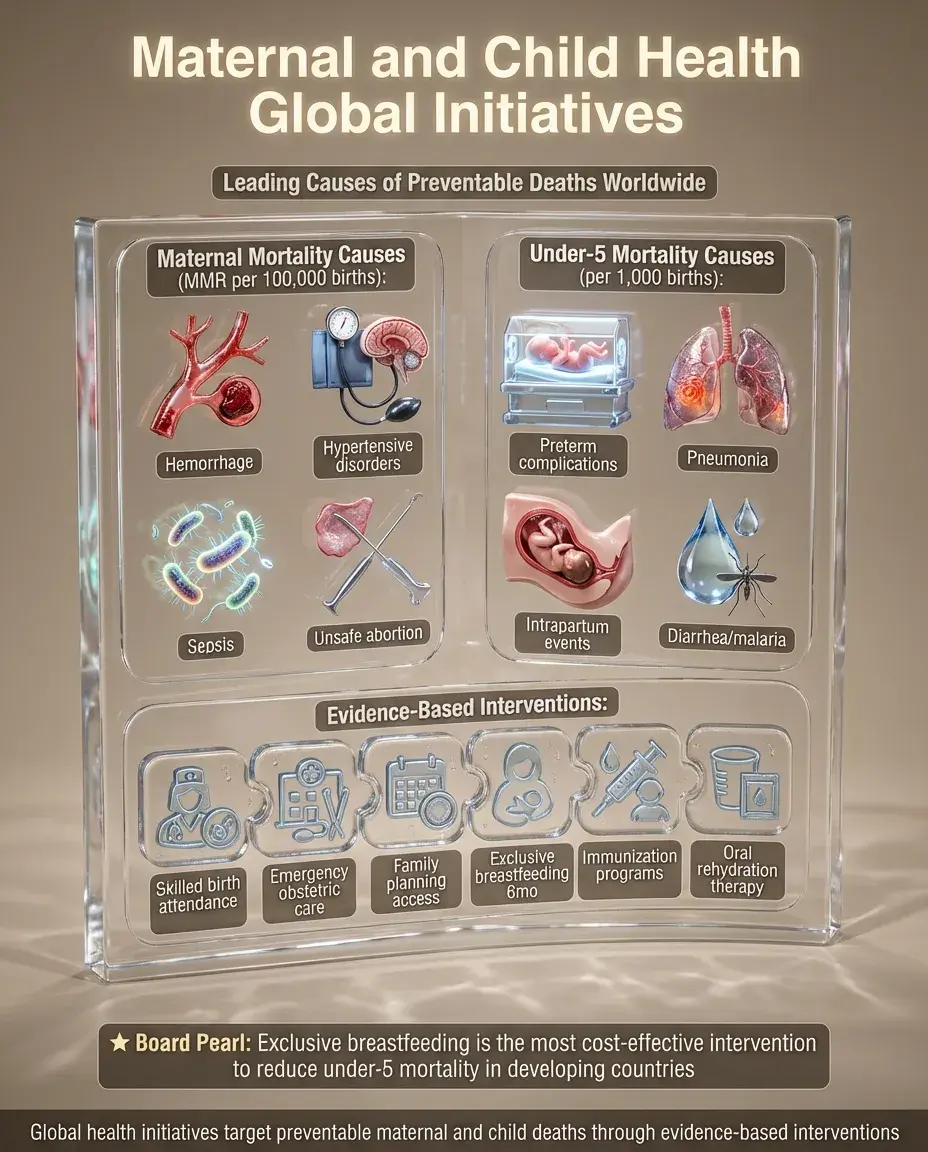
Maternal mortality ratio (MMR): maternal deaths per 100,000 live births. Leading causes globally: hemorrhage, hypertensive disorders, sepsis, unsafe abortion.
📣
Under-5 mortality rate: probability of dying between birth and 5 years per 1,000 live births. Leading causes: preterm birth complications, pneumonia, intrapartum events, diarrhea, malaria.
📣
Evidence-based interventions: skilled birth attendance, emergency obstetric care, family planning, exclusive breastfeeding for 6 months, immunization, oral rehydration therapy.
📣
Board pearl: The most cost-effective intervention to reduce under-5 mortality in developing countries is promoting exclusive breastfeeding.
Vaccine-Preventable Diseases and Immunization Programs
🔸
Expanded Programme on Immunization (EPI) targets: tuberculosis (BCG), diphtheria, tetanus, pertussis (DTP), polio, measles, hepatitis B.
🔸
Cold chain: temperature-controlled supply chain maintaining vaccines at 2-8°C from manufacturer to administration.
🔸
Vaccine coverage: percentage of target population receiving recommended vaccines. Coverage >90% needed for most herd immunity thresholds.
🔸
Board distinction: Live attenuated vaccines (MMR, varicella, yellow fever) provide longer immunity but cannot be given to immunocompromised patients; inactivated vaccines are safer but may require boosters.

Non-Communicable Disease (NCD) Prevention
🧷
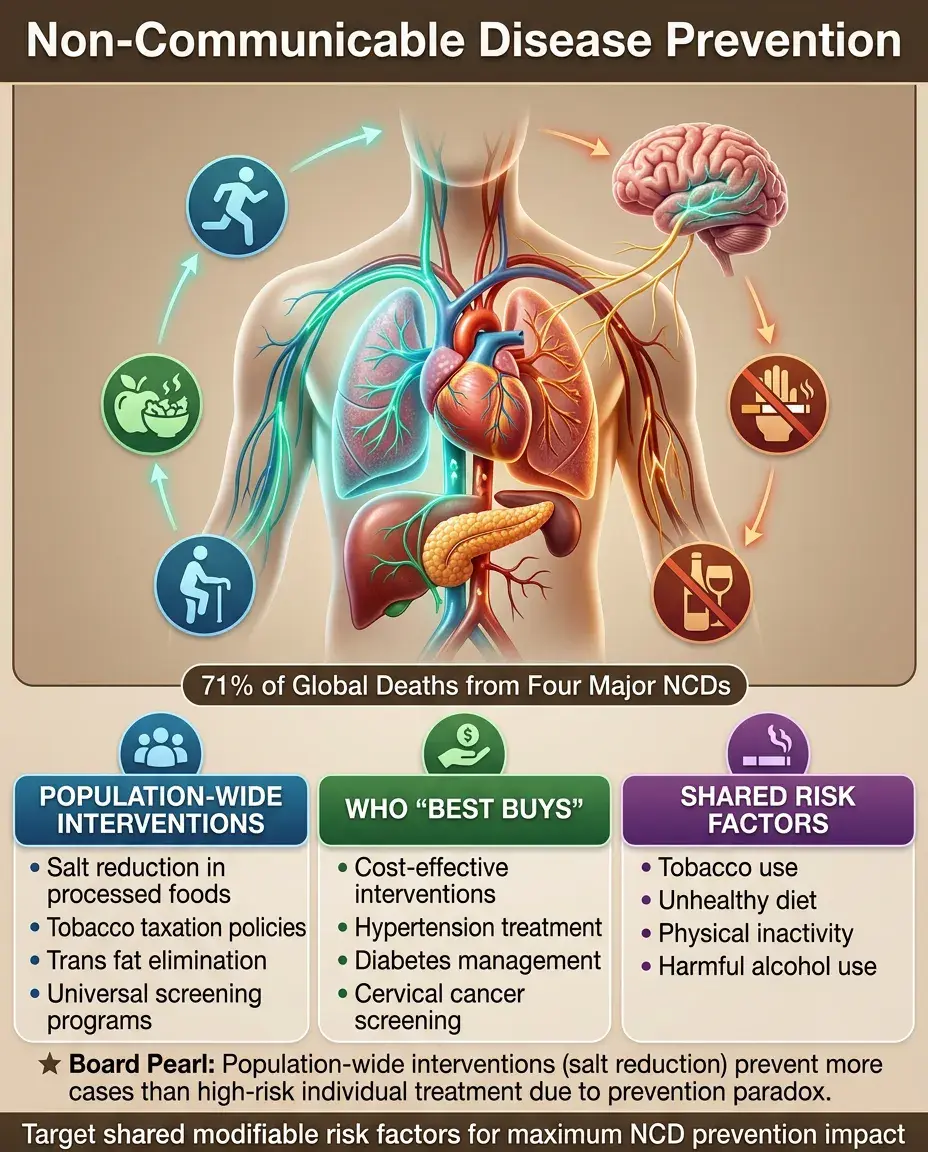
NCDs (cardiovascular disease, cancer, chronic respiratory disease, diabetes) account for 71% of global deaths.
🧷
WHO "Best Buys": cost-effective interventions including tobacco taxation, salt reduction, trans fat elimination, cervical cancer screening, treating hypertension and diabetes.
🧷
Risk factor approach: targeting shared modifiable risk factors (tobacco, unhealthy diet, physical inactivity, harmful alcohol use) that contribute to multiple NCDs.
🧷
Board pearl: Population-wide interventions (reducing salt in processed foods) have greater impact than high-risk individual approaches (treating hypertension) due to the prevention paradox.
Health Systems Strengthening
📍
WHO health system building blocks: service delivery, health workforce, health information systems, medical products/vaccines, financing, leadership/governance.
📍
Universal Health Coverage (UHC): all people have access to needed health services without financial hardship. Measured by service coverage and financial protection indicators.
📍
Task shifting: training lower-level health workers to perform tasks traditionally done by higher-level providers to address workforce shortages.
📍
Board clue: When asked about sustainable improvements in health outcomes, strengthening health systems is more effective than vertical disease-specific programs.

Disaster Response and Humanitarian Health
🔹
Disaster phases: mitigation (reducing impact), preparedness (planning), response (immediate actions), recovery (restoring normalcy).
🔹
Sphere Standards: minimum standards for humanitarian response covering water/sanitation, food security, shelter, and health services.
🔹
Priorities in acute phase: search and rescue, triage, trauma care, preventing disease outbreaks, ensuring safe water, maintaining cold chain for vaccines.
🔹
Board pearl: In disaster settings, the leading cause of mortality after the acute phase is diarrheal disease due to contaminated water and poor sanitation.

Global Health Governance and Organizations
⭐
World Health Organization (WHO): UN agency providing leadership on global health, setting norms/standards, monitoring health trends.
⭐
Key initiatives: Global Fund (HIV/AIDS, TB, malaria), GAVI (vaccine access), PEPFAR (HIV/AIDS treatment), World Bank (health system financing).
⭐
International Health Regulations (IHR): legally binding agreement requiring countries to report certain disease outbreaks and public health events.
⭐
Board distinction: WHO provides technical guidance and coordination; bilateral agencies (USAID) and multilateral organizations (World Bank) provide funding; NGOs implement programs on the ground.

Health Communication and Behavior Change
✅
Health Belief Model: behavior change depends on perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy.
✅
Stages of Change: precontemplation → contemplation → preparation → action → maintenance. Interventions must match the individual's readiness stage.
✅
Risk communication principles: be first, be right, be credible, express empathy, promote action, show respect.
✅
Board pearl: Effective health messages must be culturally appropriate, use appropriate literacy level, and address specific barriers identified through community assessment.

Program Monitoring and Evaluation
🧠
Logic model: inputs → activities → outputs → outcomes → impact. Links program resources to intended results.
🧠
Process evaluation: assesses whether program is implemented as planned (fidelity, reach, dose delivered).
🧠
Outcome evaluation: measures whether program achieves intended short-term and long-term effects.
🧠
Board distinction: Outputs are what the program does (number of vaccines given); outcomes are changes in health status (reduction in disease incidence); impact is long-term population effect (reduced mortality).

Cost-Effectiveness Analysis in Public Health
⚡
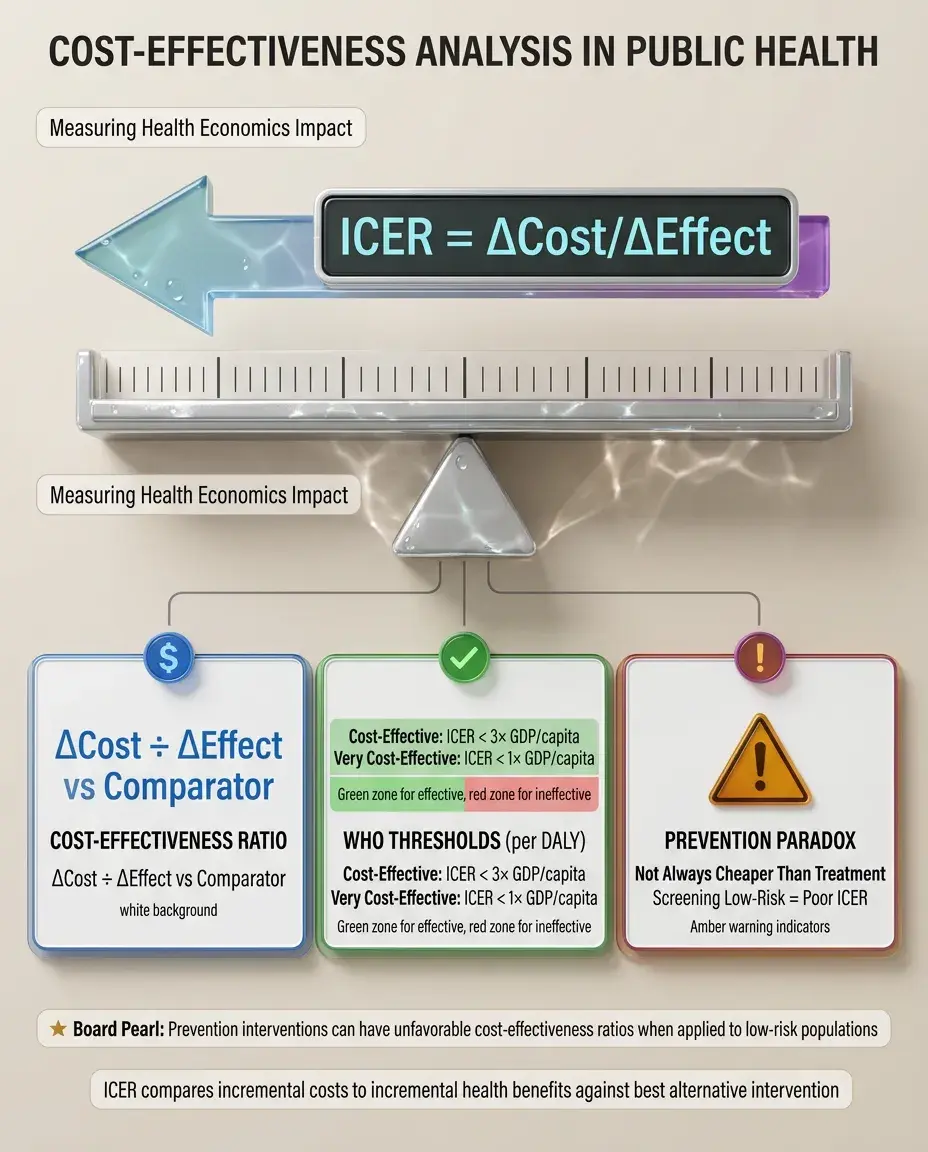
Cost-effectiveness ratio = (Cost of intervention - Cost of comparator) / (Effect of intervention - Effect of comparator).
⚡
Incremental cost-effectiveness ratio (ICER): additional cost per additional unit of health benefit compared to next best alternative.
⚡
WHO threshold: intervention is cost-effective if ICER < 3× GDP per capita per DALY averted; very cost-effective if < 1× GDP per capita.
⚡
Board pearl: Prevention is not always cheaper than treatment — some preventive interventions (screening low-risk populations) may have unfavorable cost-effectiveness ratios.
Ethics in Global Health
📌
Principles: respect for persons (autonomy, informed consent), beneficence (maximizing benefits), non-maleficence (minimizing harm), justice (fair distribution of benefits/burdens).
📌
Cultural competence: understanding and respecting cultural differences in health beliefs and practices while maintaining ethical standards.
📌
Research ethics: community engagement, fair benefit sharing, post-trial access to interventions, avoiding exploitation of vulnerable populations.
📌
Board clue: When research is conducted in resource-limited settings, the intervention being tested must be relevant and potentially accessible to the study population after the trial.

Board Question Stem Patterns
📣
Most cost-effective intervention to reduce diarrheal disease mortality → oral rehydration therapy or improved water/sanitation.
📣
Best measure of disease burden for comparing across different conditions → DALYs.
📣
Most important factor determining population health outcomes → social determinants of health.
📣
Primary prevention of cardiovascular disease at population level → tobacco control policies, not individual counseling.
📣
Leading cause of under-5 mortality globally → pneumonia and diarrheal diseases.
📣
Most critical component of outbreak response → rapid case detection and reporting.
📣
Intervention with greatest impact on maternal mortality → skilled birth attendance and emergency obstetric care.

One-Line Recap
🔸
Community and global health initiatives improve population health through prevention strategies targeting social determinants, using epidemiologic data to identify priorities, implementing evidence-based interventions across primary/secondary/tertiary prevention levels, measuring success through burden of disease metrics (DALYs/QALYs), and addressing health equity by providing resources based on need rather than equal distribution.
bottom of page