top of page

eduo
visual

Behavioral Health & Nervous System
Circadian Pacemakers: Suprachiasmatic Nucleus and Melatonin
Core Principle of Circadian Rhythms
🧷
Circadian rhythms are endogenous ~24-hour oscillations in physiology and behavior that persist even in constant environmental conditions, demonstrating their internal origin.
🧷
The suprachiasmatic nucleus (SCN) in the anterior hypothalamus serves as the master pacemaker, synchronizing peripheral clocks throughout the body to environmental light-dark cycles.
🧷
This system evolved to anticipate predictable daily changes, optimizing metabolic processes, hormone secretion, sleep-wake cycles, and cognitive performance to environmental demands.
🧷
Disruption of circadian alignment underlies jet lag, shift work disorder, and contributes to metabolic syndrome, mood disorders, and cancer risk.

Anatomy of the Suprachiasmatic Nucleus
📍
The SCN consists of paired nuclei (~20,000 neurons total) located above the optic chiasm in the anterior hypothalamus, explaining its name and strategic position to receive light input.
📍
Direct retinal input arrives via the retinohypothalamic tract (RHT), which originates from intrinsically photosensitive retinal ganglion cells containing melanopsin.
📍
These melanopsin-containing cells respond to blue light (~480nm) and project exclusively to circadian centers, separate from image-forming visual pathways.
📍
Board pearl: Blind patients with intact melanopsin cells maintain normal circadian rhythms despite complete loss of conscious vision.

Molecular Clock Mechanism
🔹
The core clock consists of transcription-translation feedback loops with ~24-hour periodicity, centered on CLOCK and BMAL1 heterodimers.
🔹
CLOCK-BMAL1 drive expression of Period (Per1, Per2) and Cryptochrome (Cry1, Cry2) genes, whose protein products accumulate and eventually inhibit their own transcription.
🔹
This negative feedback loop takes approximately 24 hours to complete, generating the circadian oscillation.
🔹
Additional loops involving REV-ERB and ROR proteins stabilize the rhythm and link it to metabolism.
🔹
Board clue: Mutations in clock genes (especially Per2) cause familial advanced sleep phase syndrome.

Melatonin Synthesis and Regulation
⭐
Melatonin synthesis follows a four-step pathway: tryptophan → 5-hydroxytryptophan → serotonin → N-acetylserotonin → melatonin.
⭐
The rate-limiting enzyme is arylalkylamine N-acetyltransferase (AANAT), whose activity increases 10-100 fold at night.
⭐
Light exposure rapidly suppresses AANAT activity within minutes, providing acute control of melatonin production.
⭐
The pineal gland lacks a blood-brain barrier, allowing rapid melatonin release into both blood and CSF.
⭐
Board pearl: Melatonin levels are highest between 2-4 AM and virtually undetectable during daylight hours in normal individuals.

Neural Pathway from Eye to Pineal
✅
Light → melanopsin retinal ganglion cells → retinohypothalamic tract → SCN → paraventricular nucleus → intermediolateral cell column (spinal cord) → superior cervical ganglion → sympathetic postganglionic fibers → pineal gland.
✅
This multisynaptic pathway explains why cervical sympathectomy (Horner syndrome) can disrupt melatonin rhythms.
✅
Norepinephrine from sympathetic terminals activates β₁-adrenergic receptors on pinealocytes → cAMP → PKA → phosphorylation of AANAT → melatonin synthesis.
✅
Board distinction: Unlike most hormones, melatonin secretion is neurally controlled rather than regulated by feedback loops.

Melatonin Receptors and Actions
🧠
MT1 and MT2 are high-affinity G-protein coupled receptors mediating most physiological effects of melatonin.
🧠
MT1 activation promotes sleep onset by inhibiting SCN neuronal firing during nighttime.
🧠
MT2 activation helps entrain circadian rhythms and regulates the timing of sleep-wake cycles.
🧠
Melatonin also acts as a potent antioxidant, scavenging free radicals independently of receptor activation.
🧠
Distribution includes SCN, cerebral arteries, immune cells, and reproductive tissues, explaining diverse effects beyond sleep.

Circadian Regulation of Physiology
⚡
Core body temperature: lowest at 4-6 AM (~36.4°C), peaks at 7-9 PM (~37.2°C) — this rhythm persists during sleep deprivation.
⚡
Cortisol: peaks at 6-8 AM (awakening response), nadir at midnight — loss of this rhythm suggests Cushing syndrome.
⚡
Growth hormone: major pulses during slow-wave sleep in first half of night.
⚡
Blood pressure: dips 10-20% during sleep (non-dipping associated with cardiovascular risk).
⚡
Board pearl: Many physiological parameters show circadian variation; timing of measurement affects interpretation.

Entrainment and Zeitgebers
📌
Zeitgebers ("time givers") are environmental cues that synchronize the internal clock to the external world.
📌
Light is the dominant zeitgeber, with morning light advancing the clock and evening light delaying it — the phase response curve.
📌
Non-photic zeitgebers include meals, exercise, social interaction, and temperature, but these are much weaker than light.
📌
Without zeitgebers, humans free-run with a period slightly longer than 24 hours (~24.2 hours), requiring daily entrainment.
📌
Board clue: Totally blind individuals often have non-24-hour sleep-wake disorder due to inability to entrain to light.

Jet Lag Pathophysiology
📣
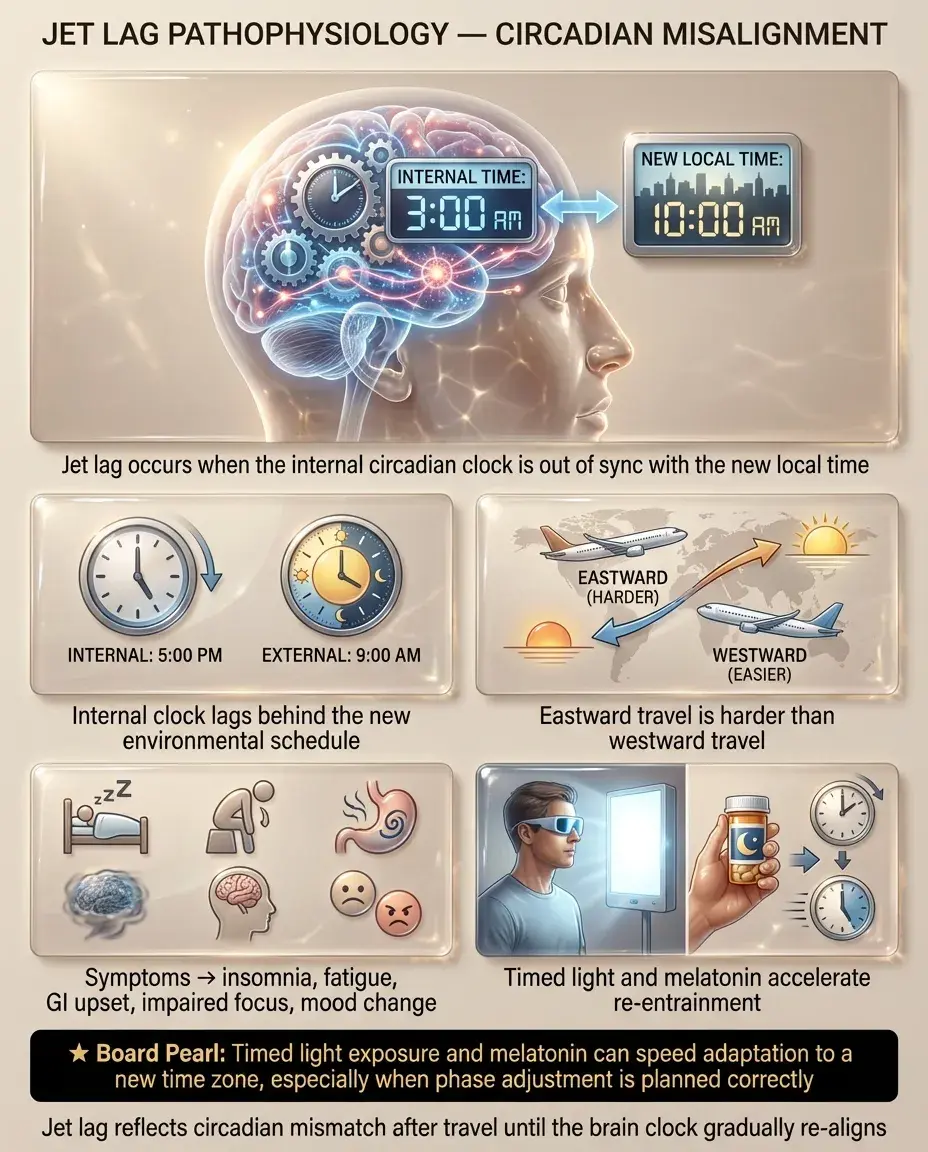
Jet lag occurs when the internal clock is misaligned with the new environmental time, causing symptoms until re-entrainment occurs.
📣
Eastward travel (phase advance) is typically harder than westward (phase delay) because the natural free-running period exceeds 24 hours.
📣
Symptoms include sleep disturbance, daytime fatigue, GI upset, cognitive impairment, and mood changes.
📣
Re-entrainment rate is approximately 1 hour/day for westward and 0.5-0.7 hours/day for eastward travel.
📣
Board pearl: Appropriately timed light exposure and melatonin can accelerate adaptation to new time zones.
Shift Work Disorder
🔸
Affects 10-30% of shift workers, characterized by insomnia during desired sleep times and excessive sleepiness during work hours.
🔸
Chronic circadian misalignment leads to increased risk of metabolic syndrome, cardiovascular disease, GI disorders, and certain cancers.
🔸
Night shift workers never fully adapt because daytime light exposure on days off re-entrains them to a day-active pattern.
🔸
Rotating shifts are particularly harmful as they prevent any stable entrainment.
🔸
Board distinction: Simple sleep deprivation improves with recovery sleep; shift work disorder persists despite adequate sleep opportunity.

Advanced and Delayed Sleep Phase Disorders
🧷
Advanced sleep phase disorder (ASPD): sleep onset before 8 PM, awakening before 4 AM — more common in elderly, linked to Per2 mutations.
🧷
Delayed sleep phase disorder (DSPD): inability to fall asleep before 2-6 AM, difficulty awakening for morning obligations — common in adolescents.
🧷
Both represent stable entrainment to the wrong phase rather than insomnia or hypersomnia.
🧷
Core body temperature minimum occurs ~2 hours before natural wake time in both conditions.
🧷
Board clue: Sleep logs showing consistent but phase-shifted sleep patterns distinguish these from irregular sleep-wake patterns.

Non-24-Hour Sleep-Wake Disorder
📍
Occurs when the circadian pacemaker free-runs without entraining to the 24-hour day, causing progressively later sleep times.
📍
Most common in totally blind individuals (~50-70% prevalence) due to absent light input to the SCN.
📍
In sighted individuals, suggests extreme delayed sleep phase or social isolation reducing zeitgeber exposure.
📍
Melatonin rhythm also free-runs, making timed administration challenging.
📍
Board pearl: Daily sleep diaries show a consistent drift of 0.5-2 hours later each day, cycling through all times over weeks.

Chronotherapy Principles
🔹
Light therapy: 10,000 lux for 30 minutes, timed based on phase response curve — morning for DSPD, evening for ASPD.
🔹
Blue light (~480nm) is most effective for circadian effects; red light has minimal impact.
🔹
Melatonin acts as a "darkness signal" — evening administration advances the clock, morning delays it (opposite of light).
🔹
Dark therapy using blue-blocking glasses can help when light avoidance is impractical.
🔹
Board distinction: Timing is critical — the same intervention can have opposite effects depending on circadian phase.

Seasonal Affective Disorder and Circadian Links
⭐
SAD represents a circadian rhythm disorder triggered by shortened winter photoperiods at higher latitudes.
⭐
Phase delay hypothesis: later dawn causes circadian delay, creating misalignment with social schedules.
⭐
Decreased light exposure reduces SCN output, affecting downstream mood-regulating regions.
⭐
Morning bright light therapy (first-line treatment) works by phase-advancing the delayed rhythm.
⭐
Board pearl: SAD improves with morning light but not evening light, supporting the phase-delay mechanism.

Circadian Disruption in Medical Conditions
✅
Alzheimer's disease: SCN degeneration causes sundowning, fragmented sleep, and loss of activity rhythms.
✅
Depression: blunted amplitude and phase advance of cortisol, temperature, and REM sleep rhythms.
✅
Bipolar disorder: extreme circadian instability; sleep deprivation can trigger mania.
✅
ICU delirium: loss of light-dark cues and continuous noise disrupt circadian organization.
✅
Board clue: Restoring robust light-dark cycles improves outcomes in ICU patients and dementia.

Metabolic Connections
🧠
Clock genes regulate key metabolic enzymes, creating circadian rhythms in glucose tolerance, insulin sensitivity, and lipid metabolism.
🧠
Insulin sensitivity peaks in morning, declines throughout day — explains worse glucose tolerance in evening.
🧠
Shift workers have increased risk of obesity, diabetes, and metabolic syndrome independent of sleep duration.
🧠
Time-restricted feeding can improve metabolic parameters by aligning eating with circadian metabolic rhythms.
🧠
Board pearl: HbA1c may underestimate glycemic control in shift workers due to circadian disruption.

Pediatric and Adolescent Considerations
⚡
Newborns lack organized circadian rhythms; SCN maturation and melatonin rhythm develop by 2-3 months.
⚡
Adolescents experience physiological phase delay due to altered sensitivity to evening light and slower accumulation of sleep pressure.
⚡
Early school start times conflict with adolescent biology, causing chronic sleep restriction and social jet lag.
⚡
ADHD symptoms worsen with circadian misalignment; many ADHD patients have delayed sleep phase.
⚡
Board distinction: Adolescent "laziness" often reflects biological phase delay, not behavioral choice.

Pharmacology and Clinical Applications
📌
Ramelteon: selective MT1/MT2 agonist for insomnia, no abuse potential unlike benzodiazepines.
📌
Tasimelteon: MT1/MT2 agonist specifically approved for non-24 disorder in blind patients.
📌
Agomelatine: MT1/MT2 agonist with 5-HT2C antagonism, used as antidepressant (not US).
📌
Suvorexant: orexin antagonist that preserves circadian sleep architecture better than GABAergic drugs.
📌
Board pearl: Melatonin receptor agonists improve sleep onset but not maintenance; useful for circadian disorders.

Board Question Stem Patterns
📣
Teenager unable to fall asleep until 3 AM despite good sleep hygiene → delayed sleep phase disorder.
📣
Blind patient with cyclical insomnia every few weeks → non-24-hour sleep-wake disorder.
📣
Night nurse with persistent fatigue despite 8 hours daytime sleep → shift work disorder.
📣
Elderly patient awakening at 3 AM, sleepy by 7 PM → advanced sleep phase disorder.
📣
Winter depression responding to morning light but not evening → seasonal affective disorder.
📣
Post-stroke patient with loss of melatonin rhythm → check for SCN or sympathetic pathway lesion.
📣
ICU patient with delirium improving with restored day-night lighting → circadian rhythm stabilization.

One-Line Recap
🔸
The suprachiasmatic nucleus serves as the master circadian pacemaker, using light input via melanopsin-containing retinal ganglion cells to synchronize molecular clocks throughout the body and regulate melatonin synthesis from the pineal gland, with disruption causing jet lag, shift work disorder, seasonal affective disorder, and contributing to metabolic and psychiatric disease.

bottom of page