top of page

eduo
visual

Gastrointestinal System
Bile acid sequestrants
Core Principle of Bile Acid Sequestrants
🧷
Bile acid sequestrants are positively charged, non-absorbable polymers that bind negatively charged bile acids in the intestinal lumen, preventing their reabsorption in the terminal ileum.
🧷
This interrupts the enterohepatic circulation of bile acids, forcing the liver to synthesize new bile acids from cholesterol via 7α-hydroxylase, thereby depleting hepatic cholesterol stores.
🧷
The liver compensates by upregulating LDL receptors (via SREBP-2 activation), increasing LDL clearance from plasma and lowering serum LDL cholesterol.
🧷
Board pearl: These drugs work entirely in the gut lumen — they are not absorbed systemically, making them safe in pregnancy and children.

Mechanism of Cholesterol Lowering
📍
Normally, 95% of bile acids are reabsorbed in the terminal ileum and recycled to the liver (enterohepatic circulation).
📍
Sequestrants create an anion exchange resin that irreversibly binds bile acids, forming an insoluble complex excreted in feces.
📍
The liver senses bile acid depletion and upregulates cholesterol 7α-hydroxylase to synthesize new bile acids from cholesterol.
📍
Hepatic cholesterol depletion → SREBP-2 activation → LDL receptor upregulation → increased LDL uptake → decreased plasma LDL.
📍
Board pearl: The entire mechanism depends on intact LDL receptors — these drugs are ineffective in homozygous familial hypercholesterolemia.

Available Agents and Dosing
🔹
Cholestyramine: oldest agent, 4-24 g/day divided BID-QID as powder mixed with liquid.
🔹
Colestipol: similar to cholestyramine, tablets or granules, 2-16 g/day.
🔹
Colesevelam: newer agent with better tolerability, 3.75 g/day as tablets or powder, can be given once daily.
🔹
All must be taken with meals when bile acids are released — timing with food is critical for efficacy.
🔹
Board distinction: Colesevelam has additional FDA approval for type 2 diabetes (modest A1c reduction ~0.5%) due to effects on glucose metabolism.

Lipid Effects and Clinical Efficacy
⭐
LDL cholesterol reduction: 15-30% (dose-dependent), maximal effect within 2 weeks.
⭐
HDL cholesterol: modest increase of 3-5%.
⭐
Triglycerides: paradoxically INCREASE by 5-15% — contraindicated if baseline TG >300 mg/dL due to risk of severe hypertriglyceridemia.
⭐
No direct effect on Lp(a) or apoB levels.
⭐
Board pearl: If a patient on a bile acid sequestrant develops worsening hypertriglyceridemia, the drug should be discontinued — this is a known class effect.

Gastrointestinal Side Effects
✅
Constipation: most common side effect (up to 30% of patients), due to binding of bile acids that normally promote colonic motility.
✅
Bloating, flatulence, and abdominal discomfort: result from altered gut flora and fermentation.
✅
Nausea and dyspepsia: especially with cholestyramine due to gritty texture and fishy odor.
✅
Steatorrhea: rare but can occur with high doses due to impaired fat absorption.
✅
Management tip: Start low and titrate slowly, ensure adequate fluid intake, consider stool softeners prophylactically.

Drug-Drug Interactions
🧠
Sequestrants can bind numerous medications in the gut, preventing their absorption: digoxin, warfarin, thyroxine, thiazide diuretics, beta-blockers, and fat-soluble vitamins (A, D, E, K).
🧠
Critical timing rule: Other medications should be taken 1 hour before or 4-6 hours after the sequestrant.
🧠
Warfarin interaction is particularly dangerous — can lead to subtherapeutic INR and thrombotic events.
🧠
May reduce absorption of oral contraceptives — alternative contraception should be considered.
🧠
Board pearl: A patient on warfarin with previously stable INR starts cholestyramine and develops DVT → suspect drug interaction.

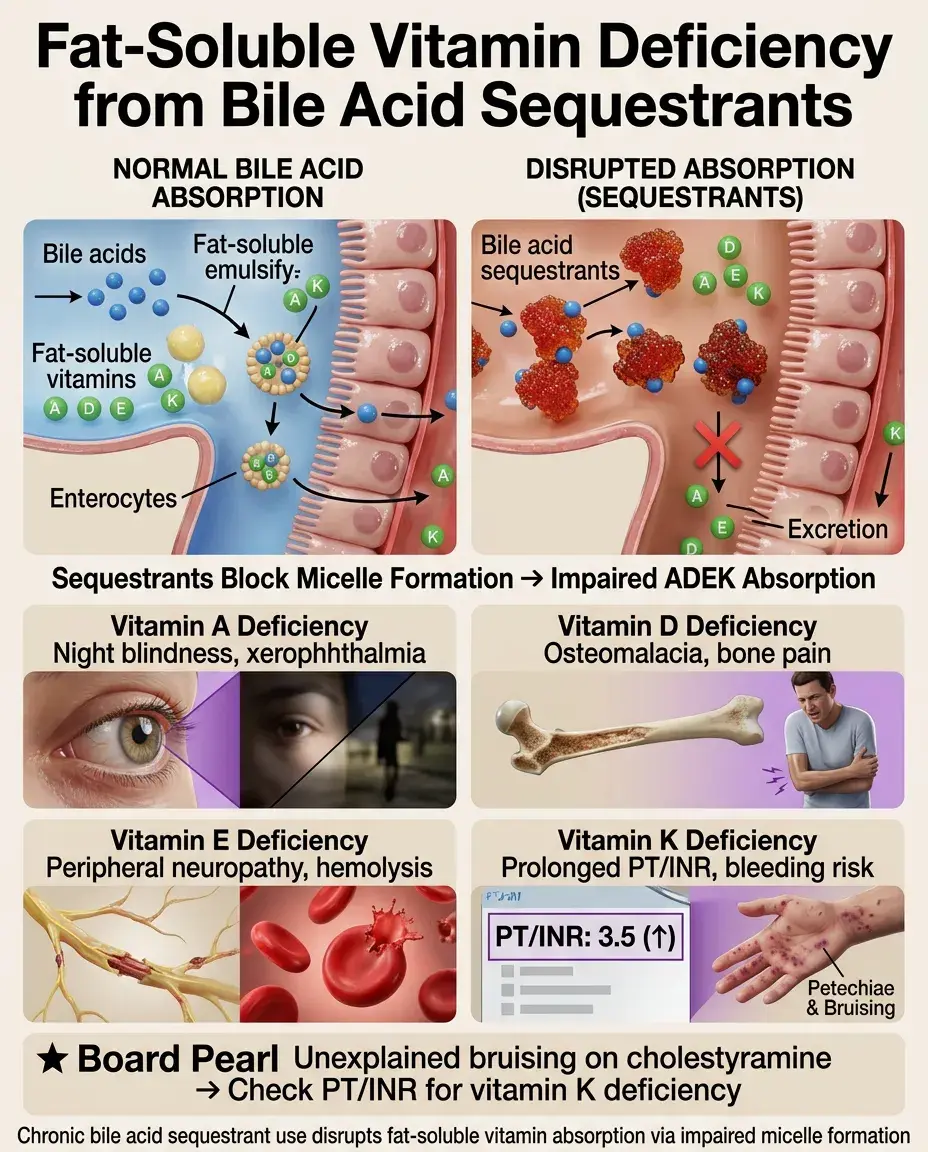
Fat-Soluble Vitamin Deficiency
⚡
Bile acids are required for micelle formation and absorption of fat-soluble vitamins (A, D, E, K) in the small intestine.
⚡
Chronic sequestrant use can lead to deficiencies: night blindness (vitamin A), osteomalacia (vitamin D), neuropathy/hemolysis (vitamin E), coagulopathy (vitamin K).
⚡
Risk is highest with high doses and prolonged therapy.
⚡
Vitamin K deficiency → prolonged PT/INR → bleeding risk, especially problematic if patient needs surgery.
⚡
Board pearl: Unexplained bruising in a patient on long-term cholestyramine → check PT/INR for vitamin K deficiency.
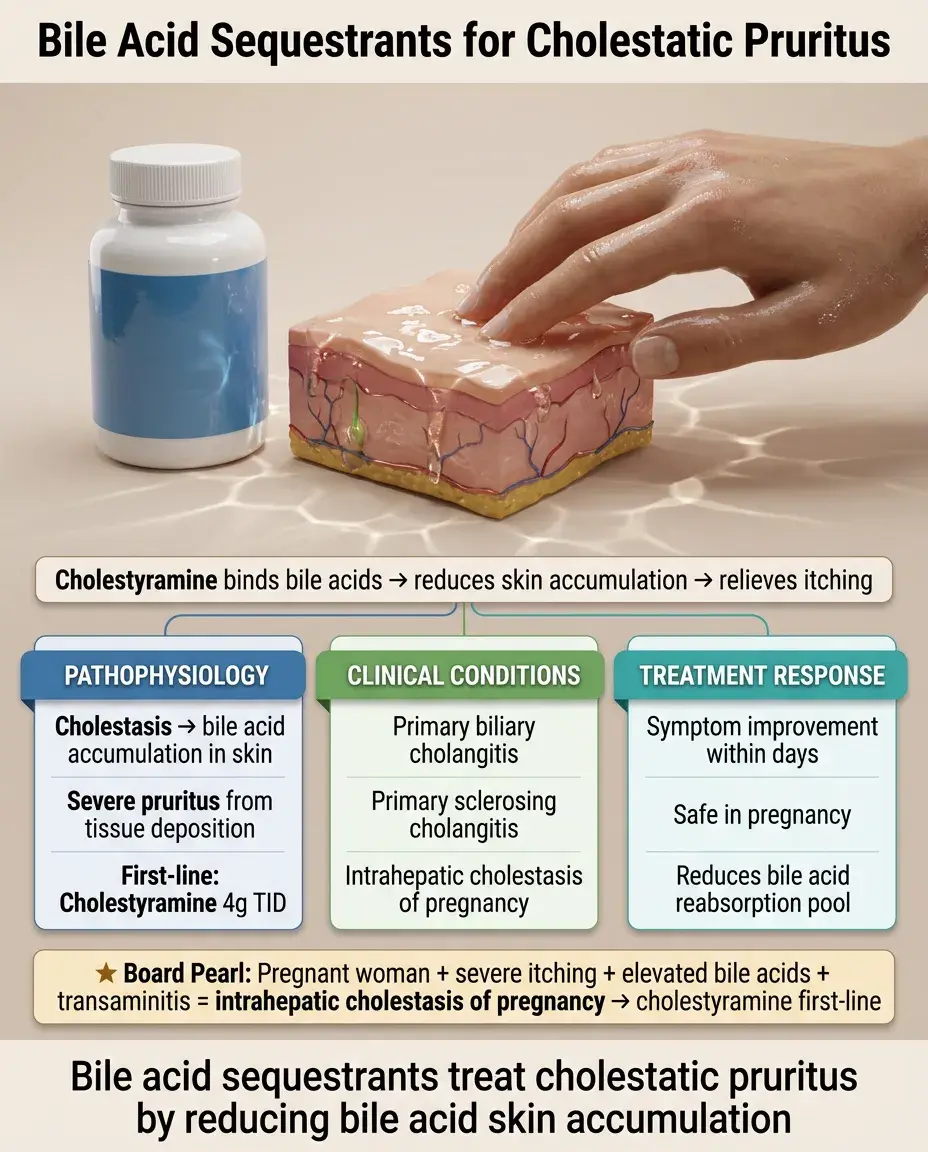
Use in Pruritus of Cholestasis
📌
Bile acid sequestrants are first-line therapy for pruritus in cholestatic liver disease (primary biliary cholangitis, primary sclerosing cholangitis, intrahepatic cholestasis of pregnancy).
📌
Pruritus is caused by bile acid accumulation in skin — sequestrants reduce the bile acid pool available for reabsorption.
📌
Cholestyramine 4 g TID is the standard regimen, with symptom improvement within days.
📌
Board pearl: Pregnant woman with severe itching, elevated bile acids, and transaminitis → intrahepatic cholestasis of pregnancy → cholestyramine is safe and effective.
Combination Therapy Strategies
📣
Sequestrants + statins: additive LDL lowering (up to 50% total reduction), different mechanisms allow synergy.
📣
Timing is critical: statin should be taken in the evening, sequestrant with breakfast and lunch to avoid interaction.
📣
Sequestrants + ezetimibe: complementary mechanisms (reduced synthesis + reduced absorption).
📣
Avoid combining with fibrates due to opposing effects on triglycerides.
📣
Board pearl: Maximum LDL reduction requires hitting multiple pathways — synthesis (statins), absorption (ezetimibe), and clearance (sequestrants).

Use in Pediatric Hyperlipidemia
🔸
Bile acid sequestrants are the only lipid-lowering drugs approved for children as young as 10 years (colesevelam).
🔸
First-line pharmacotherapy for heterozygous familial hypercholesterolemia in children after diet fails.
🔸
Safety profile is ideal for pediatrics: no systemic absorption, no effect on growth or development.
🔸
Main challenge is palatability and GI tolerability — colesevelam tablets are better tolerated than powders.
🔸
Board pearl: 12-year-old with LDL 190 mg/dL despite diet, family history of early MI → start colesevelam, not a statin.

Bile Acid Diarrhea and Sequestrants
🧷
Bile acid malabsorption causes chronic watery diarrhea due to colonic secretion stimulated by excess bile acids.
🧷
Occurs after ileal resection (Crohn's disease), radiation enteritis, or idiopathically.
🧷
Sequestrants bind excess bile acids, preventing colonic irritation and secretory diarrhea.
🧷
SeHCAT test or empiric trial of cholestyramine can establish diagnosis.
🧷
Board pearl: Patient with chronic diarrhea after ileal resection for Crohn's → empiric cholestyramine trial is both diagnostic and therapeutic.

Metabolic Effects Beyond Lipids
📍
Glucose metabolism: Colesevelam reduces HbA1c by ~0.5% through unclear mechanisms (delayed glucose absorption, incretin effects).
📍
Homocysteine: May increase levels by interfering with folate absorption — relevant for cardiovascular risk.
📍
Thyroid function: Can reduce thyroxine absorption, requiring dose adjustment in hypothyroid patients.
📍
Bile acid sequestration alters FXR and TGR5 signaling with metabolic consequences still being elucidated.
📍
Board pearl: Diabetic patient starts colesevelam for LDL → expect modest improvement in glycemic control as a bonus.

Contraindications and Precautions
🔹
Absolute contraindications: Complete biliary obstruction (no bile acids to bind), triglycerides >300 mg/dL (risk of pancreatitis from further TG elevation).
🔹
Relative contraindications: Severe constipation, major GI motility disorders, dysphagia (for powder formulations).
🔹
Use with caution in patients on multiple medications due to interaction potential.
🔹
Pregnancy category B (colesevelam) or C (cholestyramine, colestipol) — generally considered safe as not absorbed.
🔹
Board pearl: Patient with triglycerides 450 mg/dL should NOT receive bile acid sequestrants — will worsen hypertriglyceridemia.

Monitoring and Follow-up
⭐
Baseline: Lipid panel including triglycerides, liver enzymes, consider fat-soluble vitamin levels if prolonged use planned.
⭐
Follow-up lipid panel at 6-8 weeks to assess response and check for triglyceride elevation.
⭐
Annual monitoring of fat-soluble vitamins (especially vitamins A, D, K) for patients on chronic therapy.
⭐
Monitor PT/INR more frequently if on warfarin due to dual risk (drug interaction + vitamin K deficiency).
⭐
Board pearl: New-onset bleeding in a patient on chronic cholestyramine → check both PT/INR and medication timing.

Special Population Considerations
✅
Elderly: Start with lower doses due to increased susceptibility to constipation and drug interactions from polypharmacy.
✅
Pregnancy: Preferred lipid-lowering option when needed (familial hypercholesterolemia) — no systemic absorption.
✅
Chronic kidney disease: Safe option as no renal excretion required, but monitor for hyperchloremic acidosis with high doses.
✅
Liver disease: Useful for pruritus but may worsen fat malabsorption and vitamin deficiencies in advanced cirrhosis.
✅
Post-bariatric surgery: May have altered efficacy due to changed anatomy affecting bile acid circulation.

Mechanisms of Treatment Failure
🧠
Poor adherence due to GI side effects (most common cause of discontinuation).
🧠
Incorrect timing with meals — must be taken when bile acids are present.
🧠
Compensatory increase in cholesterol synthesis may limit efficacy (combine with statin to block this).
🧠
Underlying triglyceride disorder unmasked by treatment.
🧠
Malabsorption of concurrent medications leading to perceived treatment failure of other conditions.
🧠
Board pearl: Patient with "statin-resistant" hyperlipidemia starts taking cholestyramine 4 hours after their statin → likely drug interaction, not true resistance.

Cost and Formulary Considerations
⚡
Generic cholestyramine is inexpensive but poorly tolerated.
⚡
Colesevelam is more expensive but has better tolerability and once-daily dosing.
⚡
Insurance coverage varies — may require prior authorization or step therapy through older agents.
⚡
Cost-effectiveness improves in patients who cannot tolerate statins or need add-on therapy.
⚡
For bile acid diarrhea, generic cholestyramine is highly cost-effective compared to anti-diarrheal medications.

Future Directions and Novel Applications
📌
Research into bile acid sequestrants for NASH/NAFLD through FXR modulation.
📌
Potential role in colorectal cancer prevention through bile acid binding.
📌
Combination products in development to improve adherence.
📌
Novel sequestrants with higher binding capacity and selectivity.
📌
Investigation of metabolic effects beyond lipids — weight loss, inflammation, microbiome modulation.
📌
Targeted sequestrants that bind specific toxic bile acid species while preserving beneficial ones.

Board Question Stem Patterns
📣
Patient on multiple medications develops subtherapeutic drug levels → suspect timing interaction with bile acid sequestrant.
📣
Severe pruritus in pregnancy with elevated bile acids → cholestyramine for intrahepatic cholestasis of pregnancy.
📣
LDL decreased but triglycerides increased after starting new medication → bile acid sequestrant effect.
📣
Child with familial hypercholesterolemia needs treatment → bile acid sequestrant is first-line pharmacotherapy.
📣
Chronic diarrhea after ileal resection → empiric cholestyramine trial.
📣
Unexplained bleeding in patient on chronic cholestyramine → vitamin K deficiency.
📣
Diabetic with LDL elevation → colesevelam offers dual benefit.

One-Line Recap
🔸
Bile acid sequestrants are non-absorbed intestinal resins that interrupt enterohepatic circulation of bile acids, forcing hepatic cholesterol consumption for new bile acid synthesis and upregulating LDL receptors to achieve 15-30% LDL reduction, with unique applications in cholestatic pruritus and bile acid diarrhea but limited by GI side effects, drug interactions requiring careful timing, and paradoxical triglyceride elevation.

bottom of page