top of page

eduo
visual

Health Communication
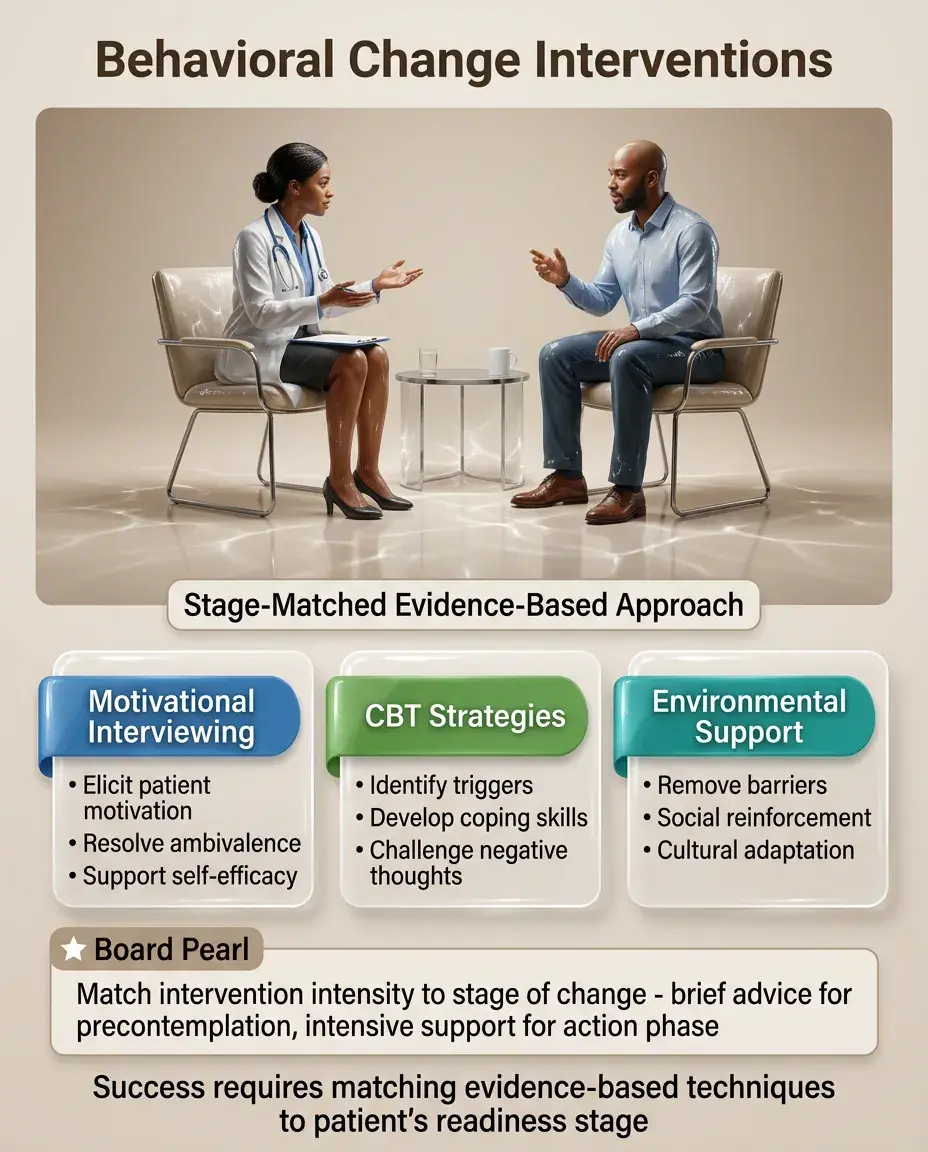
Behavioral change interventions
Core Principle of Behavioral Change Interventions
🧷
Behavioral change interventions are structured approaches designed to modify health-related behaviors by addressing the psychological, social, and environmental factors that maintain unhealthy patterns.
🧷
Effective interventions recognize that behavior change is a process, not an event, requiring different strategies at different stages of readiness.
🧷
Board questions focus on matching intervention techniques to specific behaviors and stages of change, understanding theoretical frameworks, and recognizing evidence-based approaches.
🧷
The key is understanding that successful behavior change requires more than just education — it requires addressing motivation, barriers, and reinforcement patterns.

The Transtheoretical Model (Stages of Change)
📍
Precontemplation: not considering change, unaware of problem → goal is to raise awareness, not push action.
📍
Contemplation: aware of problem, ambivalent about change → explore pros/cons, build motivation.
📍
Preparation: planning to change within 1 month → develop specific action plans, identify resources.
📍
Action: actively modifying behavior for <6 months → provide support, prevent relapse.
📍
Maintenance: sustained change for >6 months → reinforce gains, plan for high-risk situations.
📍
Board pearl: Match the intervention to the stage — giving action-oriented advice to someone in precontemplation is ineffective.

Motivational Interviewing Principles
🔹
Motivational interviewing (MI) is a patient-centered counseling style that elicits and strengthens intrinsic motivation for change.
🔹
Core principles: Express empathy, develop discrepancy between current behavior and values, roll with resistance rather than confronting it, and support self-efficacy.
🔹
Uses open-ended questions, affirmations, reflections, and summaries (OARS) to explore ambivalence.
🔹
Board distinction: MI is particularly effective for patients in contemplation stage who are ambivalent about change.
🔹
Avoid the "righting reflex" — the tendency to tell patients what to do, which typically increases resistance.

The 5 A's Framework for Brief Interventions
⭐
Ask about the behavior at every visit — screening identifies those who need intervention.
⭐
Assess readiness to change and barriers — determines appropriate intervention strategy.
⭐
Advise in a clear, personalized manner — link behavior to specific health concerns.
⭐
Assist with setting goals and developing strategies — collaborative planning increases success.
⭐
Arrange follow-up — accountability and support improve outcomes.
⭐
Board pearl: This framework is particularly tested for tobacco cessation but applies to any health behavior.
⭐
Can be delivered in 3-5 minutes, making it practical for primary care settings.

Cognitive-Behavioral Strategies
✅
Cognitive restructuring: identifying and challenging automatic negative thoughts that maintain unhealthy behaviors.
✅
Behavioral activation: scheduling pleasant activities to break cycles of avoidance and inactivity.
✅
Stimulus control: modifying environmental cues that trigger unwanted behaviors.
✅
Self-monitoring: tracking behaviors increases awareness and identifies patterns.
✅
Problem-solving training: systematic approach to overcoming barriers to change.
✅
Board clue: CBT-based interventions are first-line for many behavioral issues including smoking cessation, weight management, and substance use.

Operant Conditioning in Behavior Change
🧠
Positive reinforcement: adding rewards for desired behaviors → most effective for establishing new behaviors.
🧠
Negative reinforcement: removing unpleasant stimuli when desired behavior occurs → maintains avoidance behaviors.
🧠
Positive punishment: adding unpleasant consequences for undesired behaviors → less effective, can damage therapeutic relationship.
🧠
Extinction: removing reinforcement for undesired behaviors → initial extinction burst before behavior decreases.
🧠
Board pearl: Reinforcement schedules matter — variable ratio schedules create the most resistant-to-extinction behaviors.

Social Learning Theory Applications
⚡
Modeling: people learn by observing others → group interventions leverage peer modeling.
⚡
Self-efficacy: belief in one's ability to perform a behavior is the strongest predictor of success.
⚡
Vicarious learning: seeing similar others succeed increases confidence.
⚡
Social support: involvement of family/friends improves outcomes for most behaviors.
⚡
Board distinction: Self-efficacy is behavior-specific — success in one domain doesn't automatically transfer to others.
⚡
Interventions should provide mastery experiences, not just education, to build self-efficacy.

Harm Reduction Approaches
📌
Harm reduction accepts that complete abstinence may not be immediately achievable and focuses on reducing negative consequences.
📌
Examples: needle exchange programs, supervised injection sites, nicotine replacement for smokers not ready to quit, controlled drinking for alcohol use.
📌
Meets patients "where they are" rather than demanding immediate complete change.
📌
Board pearl: Harm reduction is evidence-based and reduces morbidity/mortality even without abstinence.
📌
Particularly important for patients in precontemplation or with multiple failed quit attempts.

Relapse Prevention Strategies
📣
Relapse is a normal part of the change process, not a failure — most people require multiple attempts.
📣
Identify high-risk situations: emotional states, social pressures, environmental cues.
📣
Develop coping strategies: behavioral alternatives, cognitive reframing, escape plans.
📣
Distinguish lapse (single instance) from relapse (return to previous pattern) → lapses don't have to become relapses.
📣
Board clue: Negative emotional states are the most common relapse trigger across all behaviors.
📣
The abstinence violation effect — catastrophic thinking after a lapse — predicts full relapse.

Brief Interventions for Substance Use
🔸
SBIRT: Screening, Brief Intervention, Referral to Treatment — systematic approach for addressing substance use in medical settings.
🔸
Brief interventions (5-15 minutes) are as effective as extended treatment for many patients with risky drinking.
🔸
Focus on raising awareness of risks, enhancing motivation, and offering practical strategies.
🔸
Use the FRAMES acronym: Feedback, Responsibility, Advice, Menu of options, Empathy, Self-efficacy.
🔸
Board pearl: Brief interventions are most effective for risky/hazardous use, less so for dependence.
🔸
Number needed to treat = 8 for reducing hazardous drinking.

Technology-Based Interventions
🧷
Text messaging: automated reminders and motivational messages → effective for medication adherence, smoking cessation.
🧷
Mobile apps: self-monitoring tools, just-in-time interventions, social support networks.
🧷
Web-based programs: accessible CBT, personalized feedback, anonymous support groups.
🧷
Teletherapy: removes geographic and mobility barriers, maintains therapeutic relationship.
🧷
Board distinction: Technology supplements but doesn't replace human connection — hybrid approaches often most effective.
🧷
Evidence strongest for adjunct use rather than stand-alone treatment.

Group-Based Interventions
📍
Group dynamics provide unique therapeutic factors: universality, instillation of hope, interpersonal learning.
📍
Peer support normalizes struggles and provides role models for successful change.
📍
Cost-effective delivery of psychoeducation and skills training.
📍
Group cohesion predicts outcomes → careful selection and group composition matters.
📍
Board pearl: Group interventions particularly effective for weight loss, smoking cessation, and substance use disorders.
📍
Contraindicated for patients with severe social anxiety or active psychosis.

Provider Communication Techniques
🔹
Use person-first language: "person with diabetes" not "diabetic" → reduces stigma and resistance.
🔹
Elicit-provide-elicit: ask permission before giving advice, check understanding afterward.
🔹
Reflective listening: paraphrase patient's statements to demonstrate understanding and clarify meaning.
🔹
Avoid confrontation and argumentation → increases defensiveness and reduces engagement.
🔹
Board clue: How something is said matters as much as what is said for behavior change.
🔹
The "spirit" of the intervention (collaborative, evocative, honoring autonomy) predicts outcomes.

Behavioral Economics Applications
⭐
Default options: making healthy choice the default → dramatically increases adoption (e.g., opt-out organ donation).
⭐
Loss framing: people more motivated by avoiding losses than achieving gains → "smoking costs $3000/year" vs "save $3000/year".
⭐
Commitment devices: public commitments or financial stakes increase follow-through.
⭐
Present bias: immediate rewards outweigh future benefits → need strategies to make long-term benefits more salient.
⭐
Board pearl: Small environmental changes (choice architecture) can produce large behavioral changes without restricting freedom.

Cultural Considerations in Interventions
✅
Cultural values influence perception of health behaviors, acceptable interventions, and therapeutic relationships.
✅
Collectivist cultures may respond better to family-involved interventions; individualist cultures to autonomy-focused approaches.
✅
Health literacy affects ability to implement complex behavior change plans → use teach-back method.
✅
Language barriers require professional interpreters, not family members, for sensitive health discussions.
✅
Board distinction: Cultural humility — ongoing self-reflection about biases — more important than cultural competence checklists.
✅
Adapt interventions to cultural context while maintaining evidence-based core components.

Specific Behavior Change Techniques
🧠
Implementation intentions: "if-then" planning → "If I feel stressed, then I will take 3 deep breaths" increases success rates.
🧠
Habit stacking: linking new behavior to established routine → "After I brush my teeth, I will take my medication."
🧠
Temptation bundling: pairing desired behavior with reward → "I can only watch Netflix while on treadmill."
🧠
Social contracting: written agreements with specific goals and consequences.
🧠
Board pearl: The more specific the plan, the more likely the behavior change — vague intentions rarely translate to action.

Measuring Behavior Change
⚡
Self-report measures: convenient but subject to social desirability bias and recall errors.
⚡
Behavioral observation: more accurate but resource-intensive and may change behavior (Hawthorne effect).
⚡
Biomarkers: objective for some behaviors (cotinine for smoking, HbA1c for diabetes management).
⚡
Ecological momentary assessment: real-time data collection reduces recall bias.
⚡
Board clue: Multiple assessment methods (triangulation) provide most accurate picture.
⚡
Process measures (attempts, strategies used) as important as outcome measures for understanding change.

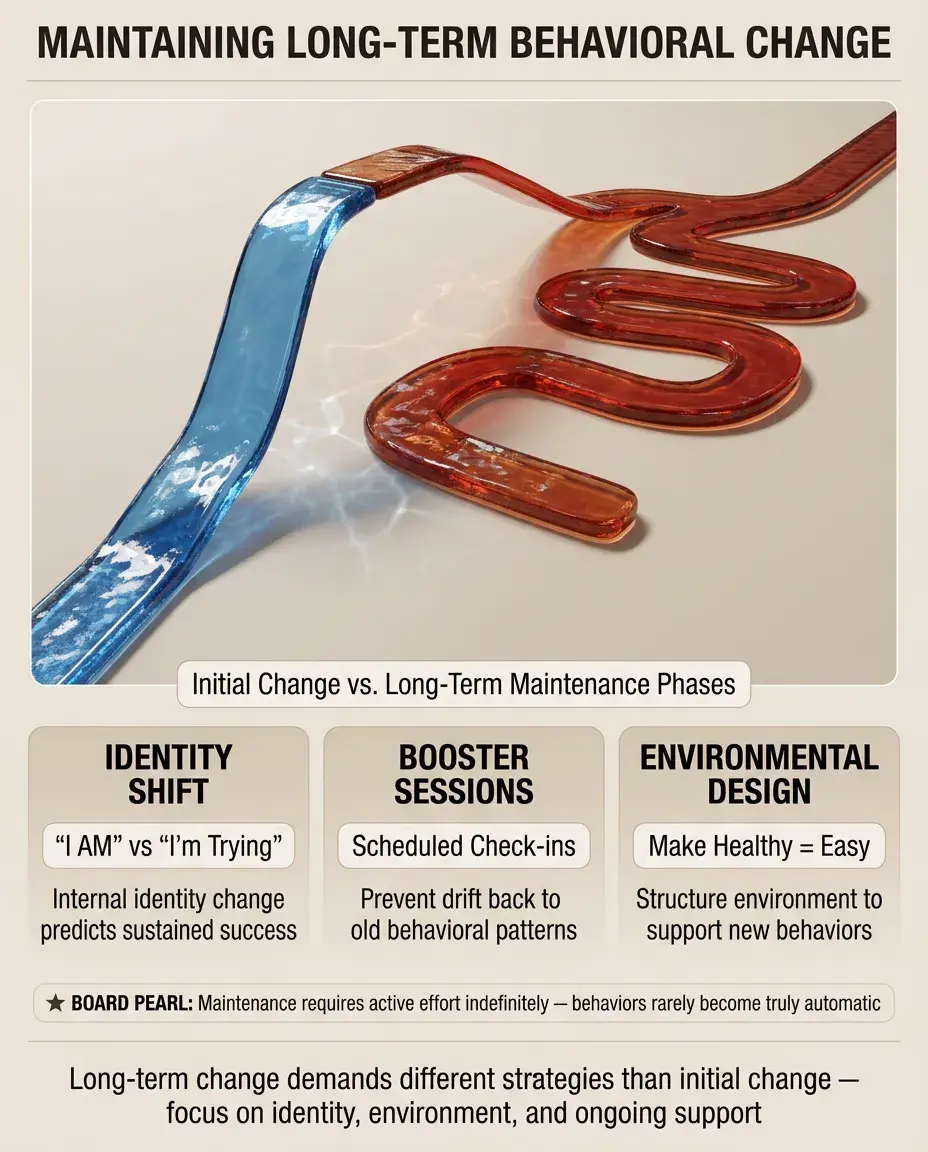
Maintaining Long-Term Change
📌
Initial change is easier than maintenance → different strategies needed for each phase.
📌
Lifestyle change requires restructuring daily routines, social networks, and coping mechanisms.
📌
Booster sessions prevent drift back to old patterns → scheduled check-ins maintain accountability.
📌
Identity shift ("I am a non-smoker" vs "I'm trying to quit") predicts long-term success.
📌
Board pearl: Maintenance requires active effort indefinitely — behaviors rarely become truly automatic.
📌
Environmental engineering to make healthy choice the easy choice crucial for sustainability.
Board Question Stem Patterns
📣
Patient "not ready to quit" smoking → precontemplation stage, use motivational interviewing, not action planning.
📣
Patient attempts change but returns to old behavior → normal part of process, explore triggers, adjust plan.
📣
Brief intervention in primary care for alcohol → evidence-based for risky drinking, use FRAMES approach.
📣
Group therapy most effective for → weight loss, smoking cessation, substance use disorders.
📣
Technology intervention as adjunct → text reminders for medication adherence, apps for self-monitoring.
📣
Cultural barrier to behavior change → adapt intervention while maintaining core evidence-based components.
📣
Physician gives unsolicited advice → likely to increase resistance, violates MI principles.

One-Line Recap
🔸
Behavioral change interventions succeed by matching evidence-based techniques (motivational interviewing, CBT strategies, brief interventions) to the patient's stage of change, leveraging psychological principles (reinforcement, self-efficacy, social learning), addressing environmental factors, and maintaining cultural sensitivity while recognizing that change is a process requiring different strategies for initiation versus maintenance.
bottom of page