top of page

eduo
visual

Behavioral Health & Nervous System
Antiepileptic Drug Mechanisms, Adverse Effects, and Teratogenicity
Core Principle of Antiepileptic Drug Mechanisms
🧷
Antiepileptic drugs (AEDs) prevent seizures by either decreasing neuronal excitation or enhancing neuronal inhibition — fundamentally tipping the balance away from synchronized hyperexcitability.
🧷
Key targets include voltage-gated sodium channels (preventing repetitive firing), voltage-gated calcium channels (reducing neurotransmitter release), GABA receptors (enhancing inhibition), and glutamate receptors (reducing excitation).
🧷
Most AEDs have multiple mechanisms, but board questions focus on the primary mechanism that explains both efficacy and side effect profile.
🧷
Understanding mechanism predicts both seizure type specificity and major toxicities.

Voltage-Gated Sodium Channel Blockade
📍
Phenytoin, carbamazepine, lamotrigine, and valproate all block voltage-gated Na⁺ channels in their inactivated state, preventing high-frequency repetitive firing.
📍
This mechanism is particularly effective for focal seizures and generalized tonic-clonic seizures but can worsen absence seizures.
📍
Use-dependent blockade means these drugs preferentially affect rapidly firing neurons while sparing normal neuronal activity.
📍
Board pearl: If a patient's absence seizures worsen after starting carbamazepine or phenytoin, the mechanism is paradoxical neuronal synchronization from Na⁺ channel blockade — switch to ethosuximide or valproate.

GABA Enhancement Mechanisms
🔹
Benzodiazepines bind to the GABA-A receptor at a site distinct from GABA, increasing frequency of chloride channel opening → enhanced inhibition.
🔹
Barbiturates (phenobarbital) also bind GABA-A receptors but increase duration of channel opening and can directly open the channel at high doses.
🔹
Vigabatrin irreversibly inhibits GABA transaminase → increased GABA concentrations in synaptic cleft.
🔹
Tiagabine blocks GABA reuptake by inhibiting GAT-1 transporter.
🔹
Board distinction: Benzodiazepines increase channel opening frequency; barbiturates increase channel opening duration.

T-Type Calcium Channel Blockade
⭐
Ethosuximide specifically blocks T-type (low-threshold) Ca²⁺ channels in thalamic neurons, disrupting the 3 Hz spike-wave discharges characteristic of absence seizures.
⭐
This mechanism explains why ethosuximide is highly effective for absence seizures but ineffective for other seizure types.
⭐
Valproate also blocks T-type channels (among other mechanisms), contributing to its broad-spectrum efficacy.
⭐
Board pearl: A child with 3 Hz spike-wave on EEG and brief staring spells → absence epilepsy → first-line treatment is ethosuximide (T-type channel blockade).

Multiple Mechanisms: Valproate and Newer Agents
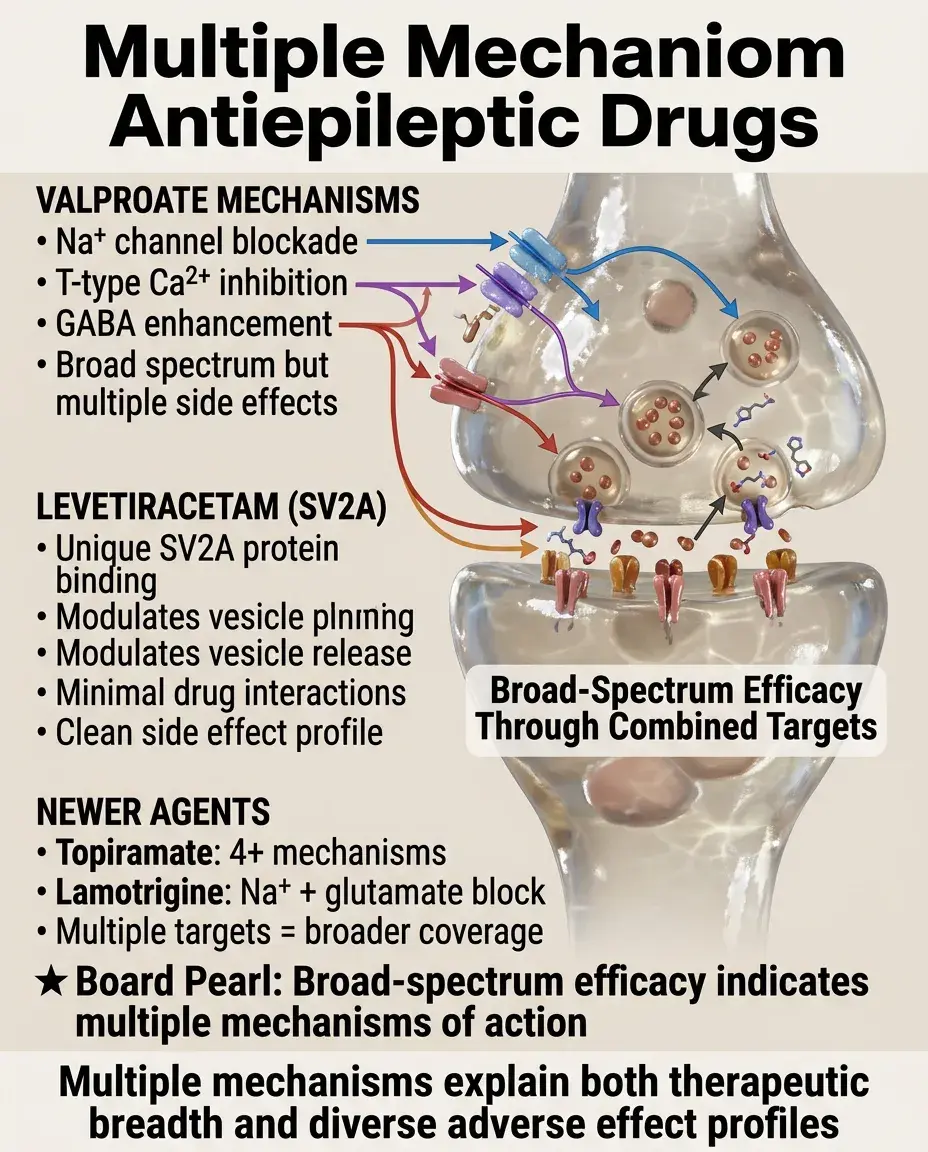
✅
Valproate: blocks Na⁺ channels, T-type Ca²⁺ channels, and increases GABA levels — explaining broad-spectrum efficacy but also diverse side effects.
✅
Levetiracetam: binds SV2A protein on synaptic vesicles, modulating neurotransmitter release — unique mechanism with minimal drug interactions.
✅
Topiramate: blocks Na⁺ channels, enhances GABA-A activity, blocks AMPA/kainate glutamate receptors, and weakly inhibits carbonic anhydrase.
✅
Lamotrigine: blocks Na⁺ channels and inhibits glutamate release.
✅
Board clue: Broad-spectrum efficacy often indicates multiple mechanisms of action.
Phenytoin: Zero-Order Kinetics and Toxicity
🧠
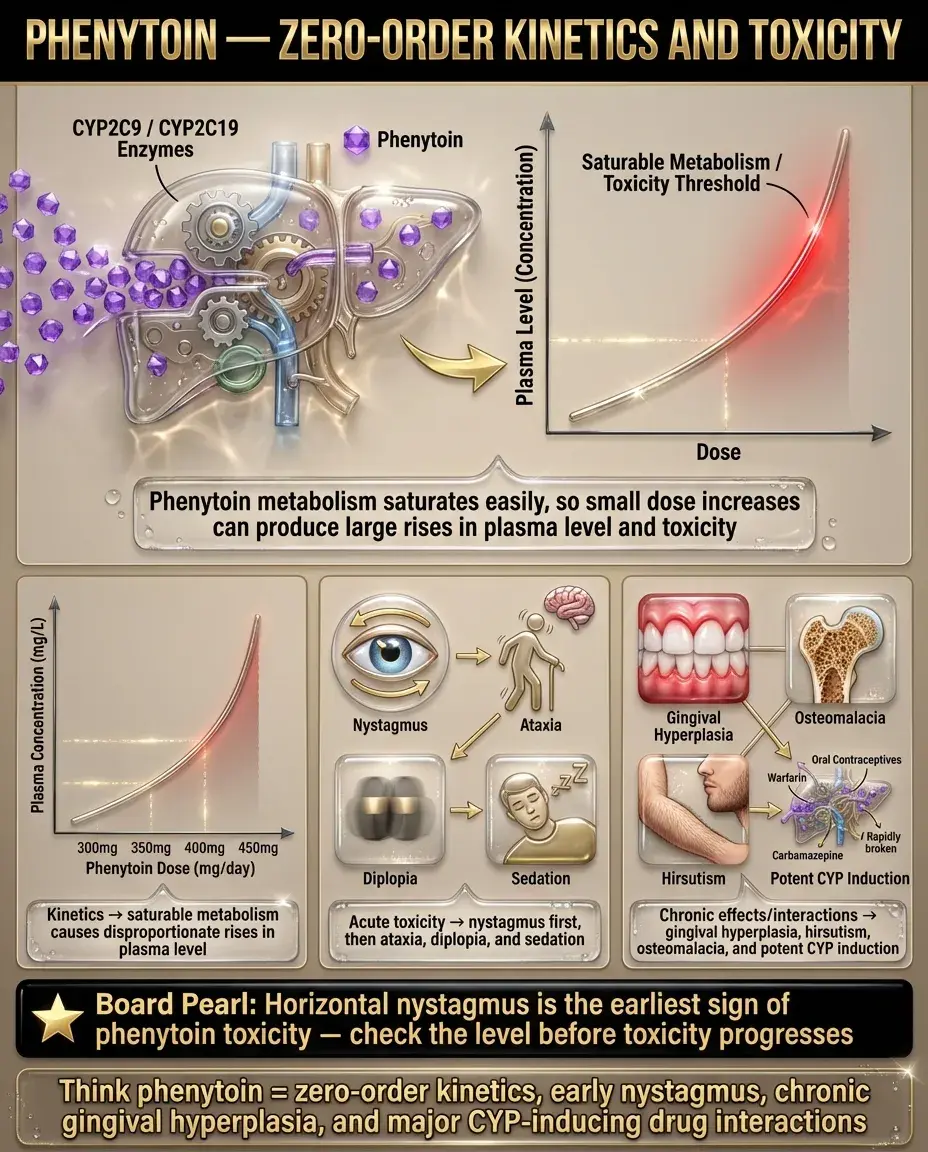
Phenytoin exhibits zero-order (saturation) kinetics at therapeutic doses — small dose increases can cause disproportionate rises in plasma levels.
🧠
Acute toxicity: nystagmus (first sign) → ataxia → diplopia → sedation.
🧠
Chronic side effects: gingival hyperplasia (20%), hirsutism, coarsening of facial features, osteomalacia (induces vitamin D metabolism).
🧠
Drug interactions: potent CYP inducer → decreases efficacy of oral contraceptives, warfarin, other drugs.
🧠
Board pearl: Horizontal nystagmus in a patient on phenytoin = early sign of toxicity → check levels.
Carbamazepine: Hematologic and Metabolic Effects
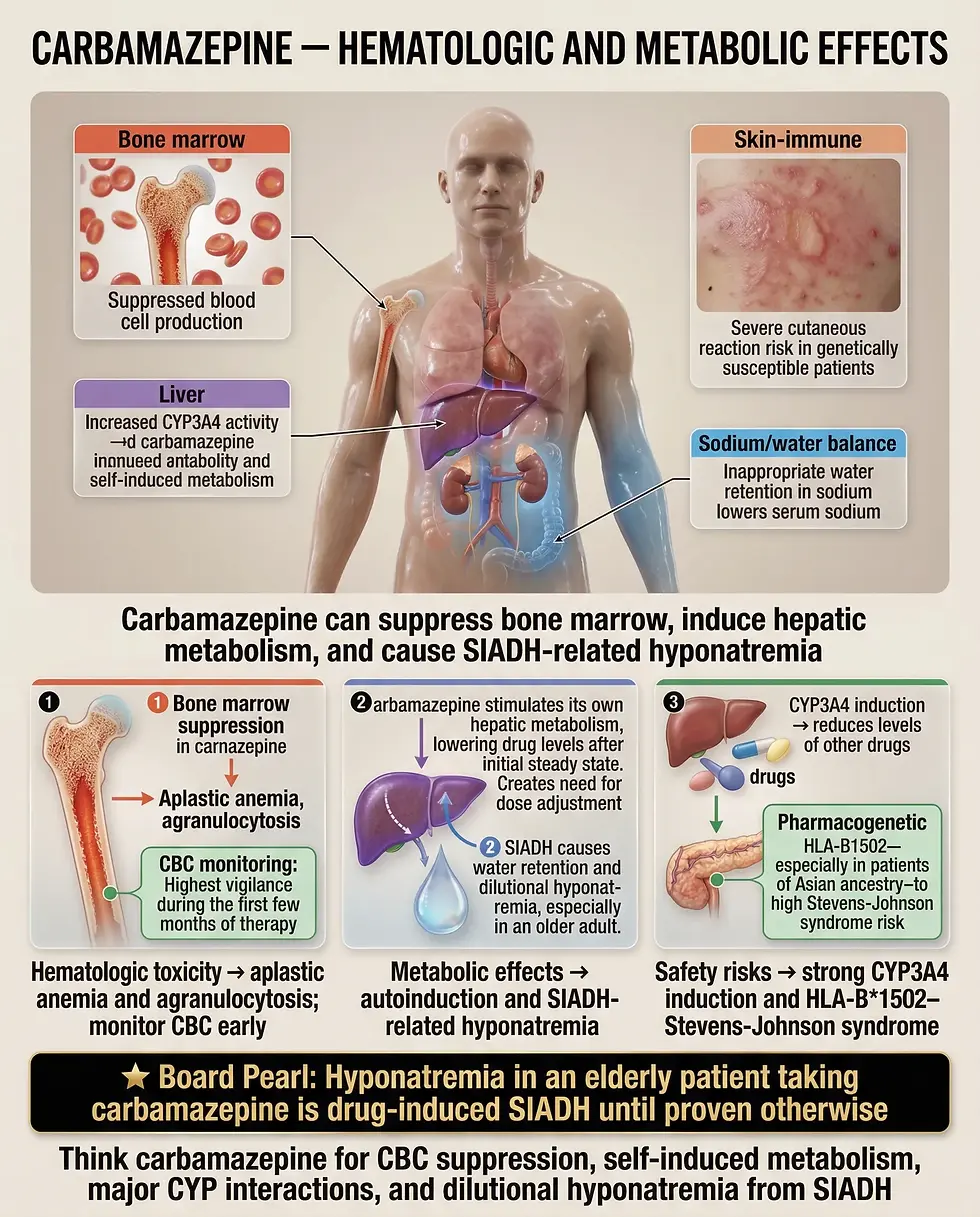
⚡
Carbamazepine can cause aplastic anemia and agranulocytosis — monitor CBC, especially in first few months.
⚡
Induces its own metabolism (autoinduction) → dose may need adjustment after steady state achieved.
⚡
Causes SIADH → hyponatremia, particularly in elderly patients.
⚡
Strong CYP3A4 inducer → multiple drug interactions.
⚡
Stevens-Johnson syndrome risk highest in HLA-B*1502 carriers (Asian ancestry).
⚡
Board distinction: Hyponatremia in elderly on carbamazepine = drug-induced SIADH.
Valproate: Hepatotoxicity and Metabolic Disturbances
📌
Hepatotoxicity ranges from transient transaminase elevation to fatal hepatic failure (highest risk in children <2 years on polytherapy).
📌
Causes hyperammonemia through inhibition of carbamoyl phosphate synthetase I → can occur with normal liver enzymes.
📌
Weight gain, alopecia, tremor are common.
📌
Thrombocytopenia and platelet dysfunction → bleeding risk.
📌
Pancreatitis is a rare but serious complication.
📌
Board pearl: Confusion in a patient on valproate with normal LFTs → check ammonia level for hyperammonemic encephalopathy.

Lamotrigine: Life-Threatening Rashes
📣
Stevens-Johnson syndrome/toxic epidermal necrolysis risk is highest with lamotrigine among all AEDs.
📣
Risk factors: rapid titration, concomitant valproate (inhibits lamotrigine metabolism), and previous AED rashes.
📣
Must use slow titration schedule — even slower when combined with valproate.
📣
Benign rash occurs in ~10%, but any rash requires careful evaluation given SJS risk.
📣
Board pearl: New AED rash with mucosal involvement → stop drug immediately and hospitalize for possible Stevens-Johnson syndrome.

Topiramate: Cognitive and Metabolic Effects
🔸
Cognitive side effects: word-finding difficulty, psychomotor slowing, memory impairment — "dopamax" nickname reflects these effects.
🔸
Carbonic anhydrase inhibition → metabolic acidosis, kidney stones (calcium phosphate), acute myopia/angle-closure glaucoma.
🔸
Weight loss (unlike most AEDs) — sometimes used off-label for this effect.
🔸
Oligohidrosis and hyperthermia, especially in children.
🔸
Board clue: Word-finding difficulty + kidney stones in epilepsy patient = topiramate side effects.

Benzodiazepines and Barbiturates: Sedation and Dependence
🧷
Both cause dose-dependent CNS depression: anxiolysis → sedation → hypnosis → anesthesia → coma → death.
🧷
Tolerance develops to sedative effects but not anticonvulsant effects.
🧷
Physical dependence with withdrawal seizures upon abrupt discontinuation.
🧷
Barbiturates induce CYP enzymes; benzodiazepines generally do not.
🧷
Board distinction: Flumazenil reverses benzodiazepine overdose but can precipitate seizures in dependent patients; no reversal agent exists for barbiturates.

Neural Tube Defects: Valproate and Carbamazepine
📍
Valproate has the highest teratogenic risk among AEDs: 1–2% risk of spina bifida (vs 0.05% baseline).
📍
Mechanism: interference with folate metabolism during neural tube closure (days 21–28).
📍
Carbamazepine also increases neural tube defect risk but less than valproate.
📍
High-dose folic acid (4–5 mg daily) recommended before conception and during pregnancy, though doesn't eliminate risk.
📍
Board pearl: Woman of childbearing age with epilepsy → avoid valproate if possible; if necessary, counsel about risks and ensure folic acid supplementation.

Fetal Hydantoin Syndrome
🔹
Phenytoin causes a recognizable pattern of malformations in ~10% of exposed fetuses.
🔹
Features: craniofacial abnormalities (wide-set eyes, broad nasal bridge, cleft lip/palate), digit hypoplasia (especially 5th digit), nail hypoplasia, growth restriction.
🔹
Developmental delay and intellectual disability in some cases.
🔹
Risk appears dose-dependent but no clear safe threshold.
🔹
Board clue: Infant with nail hypoplasia and distinctive facies born to mother with epilepsy = fetal hydantoin syndrome.

Newer AEDs and Pregnancy
⭐
Levetiracetam and lamotrigine have the most favorable pregnancy data among newer AEDs — becoming preferred choices for women of childbearing age.
⭐
Topiramate associated with increased risk of cleft lip/palate and small for gestational age.
⭐
All AEDs carry some teratogenic risk; goal is seizure control with lowest effective dose of safest medication.
⭐
Pregnancy registries continue to collect data on newer agents.
⭐
Board principle: Uncontrolled seizures pose greater risk to fetus than AED exposure — don't stop AEDs abruptly in pregnancy.

Vitamin Interactions and Bone Health
✅
Enzyme-inducing AEDs (phenytoin, carbamazepine, phenobarbital) increase vitamin D catabolism → osteomalacia, osteoporosis.
✅
These drugs also induce folate metabolism → megaloblastic anemia (without neuropathy, unlike B12 deficiency).
✅
Valproate can cause carnitine deficiency → hepatic encephalopathy, especially in children.
✅
Vitamin K deficiency in neonates exposed to enzyme-inducing AEDs → hemorrhagic disease of newborn.
✅
Board pearl: Epilepsy patient with elevated alkaline phosphatase and bone pain = AED-induced osteomalacia → check vitamin D levels.

Drug-Drug Interactions
🧠
Enzyme inducers (phenytoin, carbamazepine, phenobarbital): decrease levels of oral contraceptives, warfarin, cyclosporine, HIV protease inhibitors.
🧠
Enzyme inhibitors (valproate): increase levels of lamotrigine, phenobarbital → toxicity risk.
🧠
Protein binding displacement: valproate displaces phenytoin from albumin → increased free phenytoin.
🧠
Levetiracetam has no significant drug interactions — major advantage.
🧠
Board scenario: Breakthrough seizures after starting oral contraceptives = enzyme induction reducing AED levels.

Status Epilepticus Treatment Sequence
⚡
First-line: IV lorazepam (preferred) or diazepam — rapid onset, effective termination of most seizures.
⚡
Second-line: IV phenytoin/fosphenytoin, valproate, or levetiracetam — given as loading dose for sustained control.
⚡
Third-line (refractory status): propofol, midazolam infusion, or phenobarbital — requires intubation and ICU monitoring.
⚡
Mechanism consideration: benzodiazepines for immediate GABA enhancement, then Na⁺ channel blockers for sustained control.
⚡
Board pearl: No IV access in seizing patient → intramuscular midazolam or rectal diazepam are alternatives to IV benzodiazepines.

Therapeutic Drug Monitoring
📌
Phenytoin: narrow therapeutic index, zero-order kinetics → monitor levels, adjust for albumin (free phenytoin = measured level ÷ (0.2 × albumin + 0.1)).
📌
Carbamazepine: monitor for autoinduction effect, check levels and CBC.
📌
Valproate: levels less useful due to poor correlation with efficacy; monitor LFTs, CBC, ammonia if symptomatic.
📌
Newer AEDs: routine monitoring generally not needed except for adherence or toxicity concerns.
📌
Board distinction: Only correct phenytoin levels for low albumin; other AED levels don't require correction.

Board Question Stem Patterns
📣
Child with staring spells and 3 Hz spike-wave → absence seizures → ethosuximide.
📣
Horizontal nystagmus in epilepsy patient → phenytoin toxicity.
📣
Epilepsy patient with word-finding difficulty and kidney stones → topiramate.
📣
Pregnant woman with epilepsy → levetiracetam or lamotrigine preferred; high-dose folic acid regardless.
📣
Hyponatremia in elderly on AED → carbamazepine-induced SIADH.
📣
Breakthrough seizures after starting new medication → check for enzyme induction.
📣
Confusion with normal LFTs on valproate → check ammonia.
📣
Infant with nail hypoplasia born to epileptic mother → fetal hydantoin syndrome.

One-Line Recap
🔸
Antiepileptic drugs work by blocking voltage-gated channels (Na⁺ or Ca²⁺) or enhancing GABA inhibition, with drug choice guided by seizure type and side effect profile, major concerns including teratogenicity (highest with valproate), drug interactions (worst with enzyme inducers), and specific toxicities (phenytoin nystagmus, carbamazepine SIADH, lamotrigine rash, valproate hepatotoxicity).

bottom of page