top of page

eduo
visual

Respiratory System
Alveolar gas equation
Core Principle of the Alveolar Gas Equation
🧷
The alveolar gas equation calculates the partial pressure of oxygen in the alveoli (PAO₂), establishing the theoretical maximum oxygen available for diffusion into the blood.
🧷
It accounts for the fact that oxygen is consumed while CO₂ is added to alveolar gas, creating a steady-state balance between inspired oxygen and metabolic demands.
🧷
The equation bridges atmospheric oxygen delivery to cellular oxygen consumption by quantifying the first step in the oxygen cascade.
🧷
Understanding PAO₂ is essential for calculating the A-a gradient, which distinguishes between normal gas exchange and pathologic barriers to diffusion.

The Alveolar Gas Equation Formula
📍
PAO₂ = FiO₂(Patm − PH₂O) − PaCO₂/RQ
📍
FiO₂ = fraction of inspired oxygen (0.21 on room air)
📍
Patm = atmospheric pressure (760 mmHg at sea level)
📍
PH₂O = water vapor pressure (47 mmHg at body temperature)
📍
PaCO₂ = arterial CO₂ pressure (normally 40 mmHg)
📍
RQ = respiratory quotient (typically 0.8 for mixed diet)
📍
Board pearl: At sea level on room air, this simplifies to PAO₂ ≈ 150 − 1.25(PaCO₂), yielding a normal PAO₂ of approximately 100 mmHg.

The Respiratory Quotient (RQ)
🔹
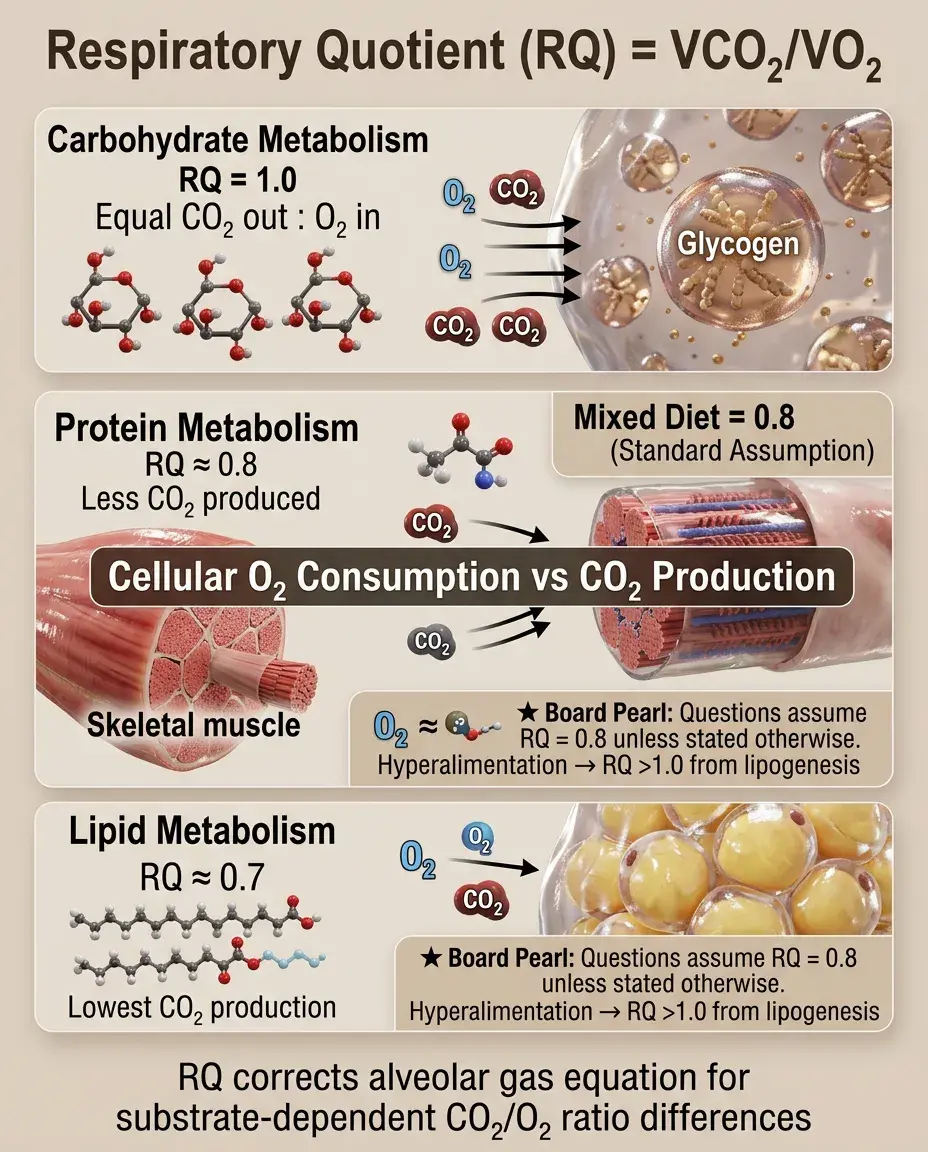
RQ = VCO₂/VO₂, representing the ratio of CO₂ production to O₂ consumption at the cellular level.
🔹
RQ varies by metabolic substrate: carbohydrates = 1.0, proteins ≈ 0.8, lipids ≈ 0.7, mixed diet ≈ 0.8.
🔹
In the alveolar gas equation, RQ corrects for the fact that less CO₂ is produced than O₂ consumed (except with pure carbohydrate metabolism).
🔹
Board clue: Questions typically assume RQ = 0.8 unless specifically stated otherwise.
🔹
During hyperalimentation with high glucose loads, RQ can exceed 1.0 due to lipogenesis, increasing CO₂ production.
The Alveolar-Arterial (A-a) Gradient
⭐
A-a gradient = PAO₂ − PaO₂, where PaO₂ is measured from arterial blood gas.
⭐
Normal A-a gradient = Age/4 + 4 (in mmHg), typically <10-15 mmHg in young healthy adults.
⭐
The gradient represents the efficiency of oxygen transfer across the alveolar-capillary membrane.
⭐
An elevated A-a gradient indicates impaired gas exchange: V/Q mismatch, diffusion impairment, or right-to-left shunt.
⭐
A normal A-a gradient with hypoxemia suggests hypoventilation or low inspired oxygen concentration.

Causes of Elevated A-a Gradient
✅
V/Q mismatch: most common cause (pneumonia, pulmonary embolism, COPD, asthma)
✅
Shunt: blood bypasses ventilated alveoli (intracardiac shunt, pulmonary AVM, severe consolidation)
✅
Diffusion impairment: thickened alveolar-capillary membrane (interstitial lung disease, pulmonary edema)
✅
Board distinction: Shunt does not correct with 100% O₂; V/Q mismatch improves significantly with supplemental oxygen.
✅
Right-to-left shunts cause hypoxemia out of proportion to the radiographic findings.

Hypoxemia with Normal A-a Gradient
🧠
Hypoventilation: increased PaCO₂ displaces alveolar oxygen (opioid overdose, neuromuscular weakness)
🧠
Low inspired oxygen: high altitude or equipment malfunction
🧠
Key principle: When PaCO₂ rises, PAO₂ falls by approximately 1.25 mmHg per 1 mmHg increase in CO₂.
🧠
These conditions represent inadequate oxygen delivery to the alveoli rather than impaired gas exchange.
🧠
Board pearl: Normal A-a gradient + hypoxemia + hypercapnia = hypoventilation until proven otherwise.

High Altitude Physiology and the Alveolar Gas Equation
⚡
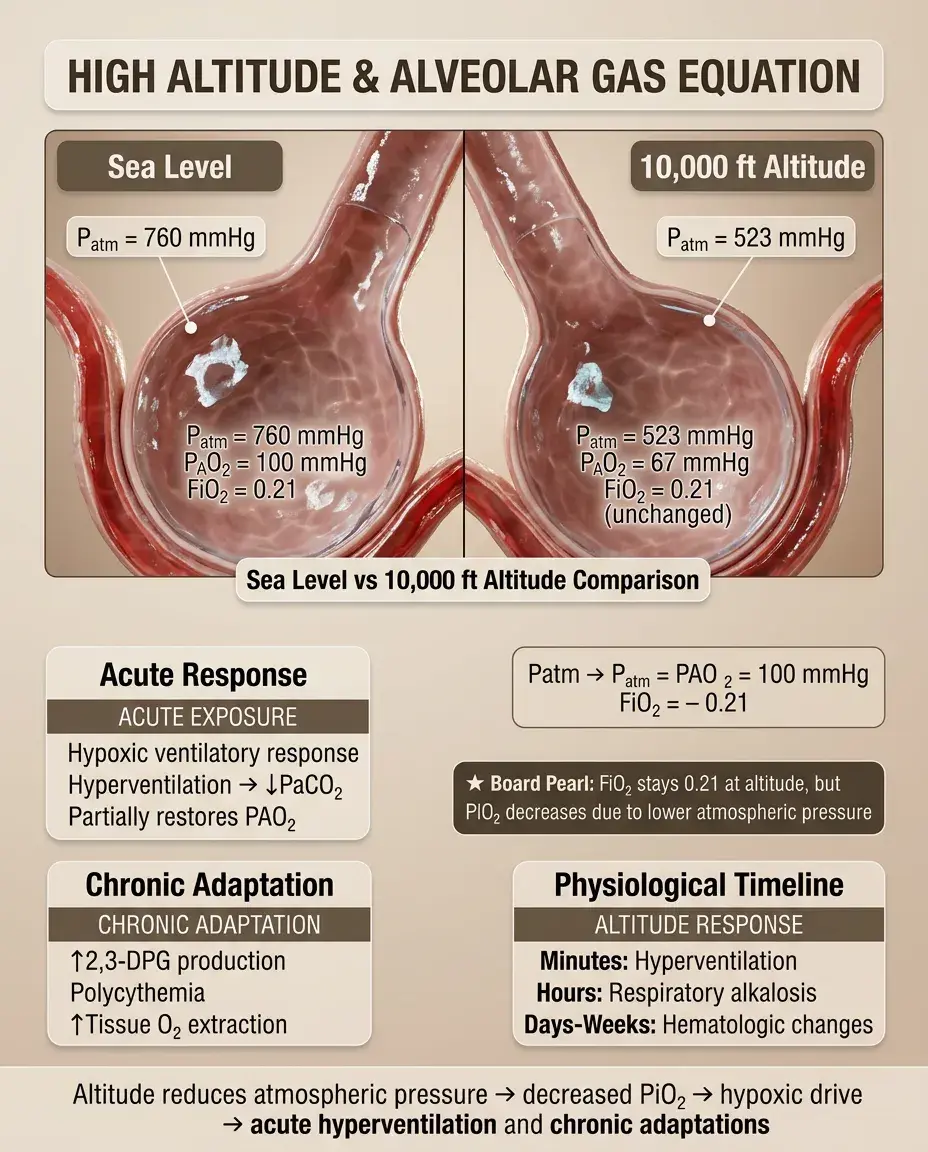
At altitude, decreased atmospheric pressure reduces PAO₂ despite unchanged FiO₂.
⚡
Example: At 10,000 feet, Patm ≈ 523 mmHg → PAO₂ ≈ 67 mmHg on room air.
⚡
Acute exposure causes hypoxic ventilatory response → hyperventilation → decreased PaCO₂ → partially restored PAO₂.
⚡
Chronic adaptation includes increased 2,3-DPG, polycythemia, and improved tissue oxygen extraction.
⚡
Board clue: Altitude-related questions often test the concept that FiO₂ remains 0.21 but PiO₂ decreases.
Effects of Supplemental Oxygen
📌
Increasing FiO₂ directly increases PAO₂ in a linear relationship.
📌
Each 10% increase in FiO₂ adds approximately 50 mmHg to PAO₂ (at sea level).
📌
On 100% oxygen: PAO₂ ≈ 663 mmHg (after accounting for water vapor and CO₂).
📌
Supplemental oxygen corrects hypoxemia from V/Q mismatch but has minimal effect on true shunt.
📌
Board pearl: Failure to improve PaO₂ >500 mmHg on 100% O₂ suggests shunt fraction >30%.

Clinical Application: Assessing Oxygenation Failure
📣
Step 1: Calculate PAO₂ using the alveolar gas equation
📣
Step 2: Calculate A-a gradient (PAO₂ − PaO₂)
📣
Step 3: If A-a gradient elevated → gas exchange problem (V/Q mismatch, shunt, diffusion)
📣
Step 4: If A-a gradient normal → ventilation problem (hypoventilation) or low FiO₂
📣
This systematic approach distinguishes lung parenchymal disease from pump failure.
📣
Board approach: ABG + room air + hypoxemia → always calculate A-a gradient first.

The PaO₂/FiO₂ Ratio
🔸
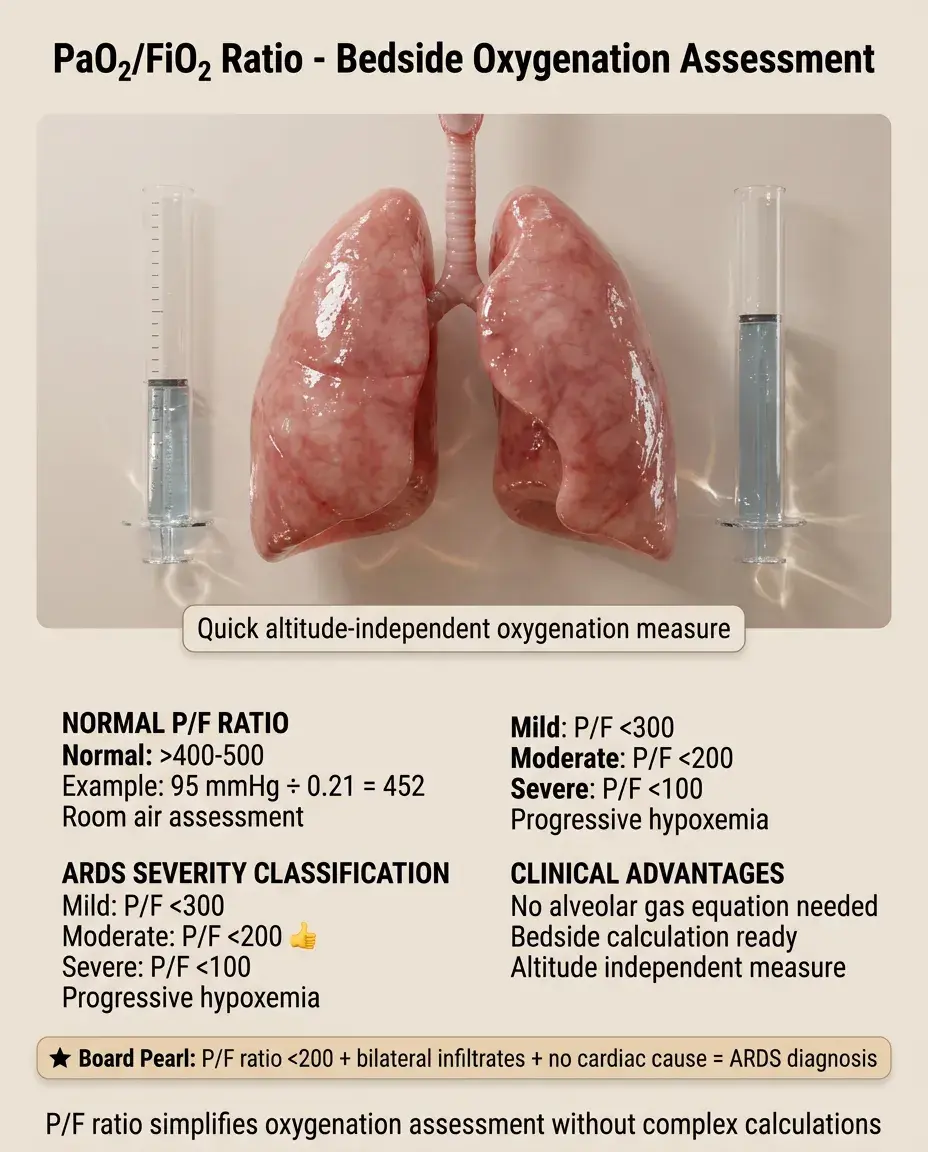
P/F ratio = PaO₂/FiO₂, a quick bedside assessment of oxygenation independent of altitude.
🔸
Normal P/F ratio >400-500 on room air (example: PaO₂ 95/FiO₂ 0.21 = 452).
🔸
ARDS definition: P/F ratio <300 (mild), <200 (moderate), <100 (severe).
🔸
Unlike A-a gradient, P/F ratio doesn't require the alveolar gas equation calculation.
🔸
Board pearl: P/F ratio <200 + bilateral infiltrates + no cardiac cause = ARDS.
Diffusion Limitation and the Alveolar Gas Equation
🧷
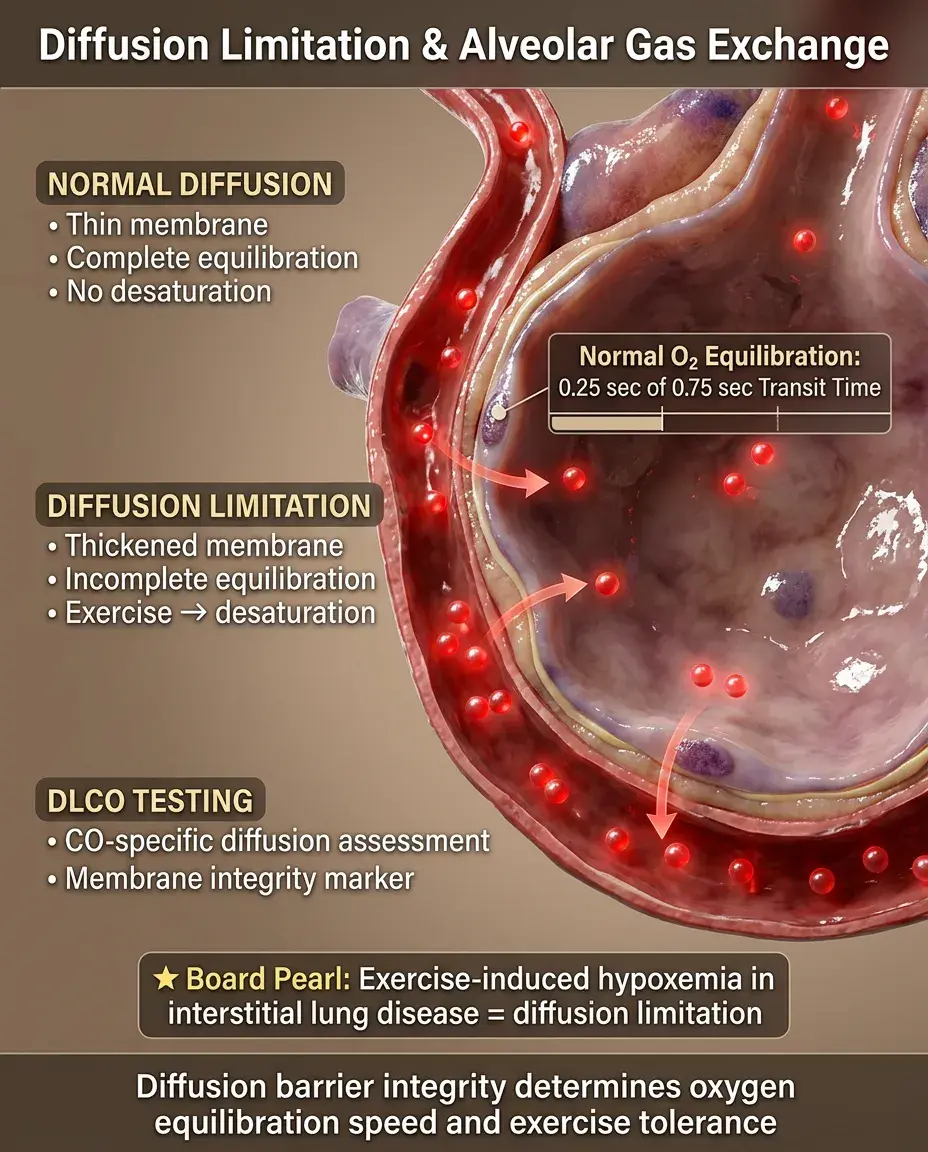
Normal oxygen equilibrates between alveolar gas and capillary blood within 0.25 seconds (of 0.75 second transit time).
🧷
Diffusion limitation occurs when this equilibration is incomplete due to membrane thickening or decreased transit time.
🧷
Exercise unmasks diffusion limitation by reducing capillary transit time → desaturation with exertion.
🧷
Carbon monoxide diffusion capacity (DLCO) specifically tests diffusion barrier integrity.
🧷
Board clue: Exercise-induced hypoxemia in interstitial lung disease = diffusion limitation.
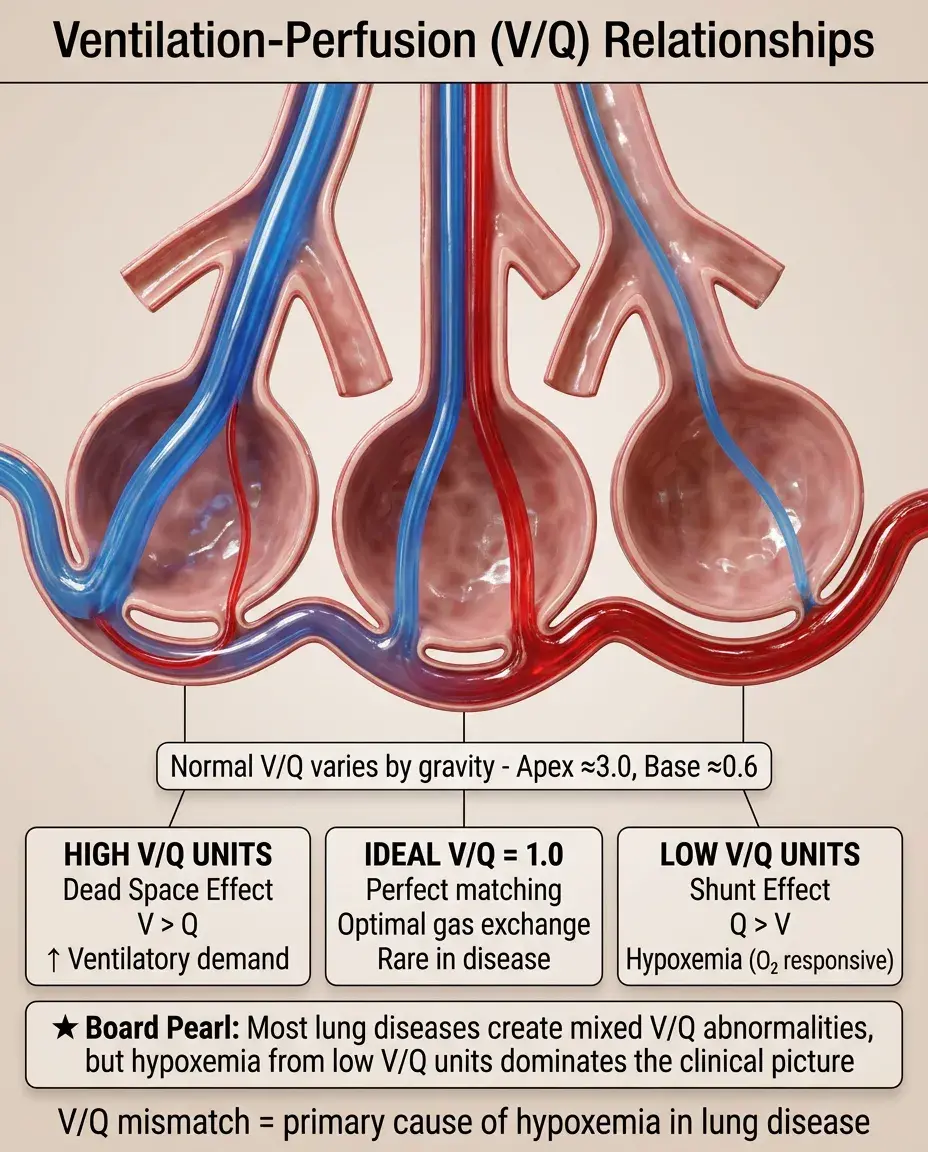
Ventilation-Perfusion Relationships
📍
Ideal V/Q ratio = 1.0, but physiologic V/Q varies from apex (≈3.0) to base (≈0.6) due to gravity.
📍
Low V/Q units (perfusion > ventilation) cause hypoxemia that responds to supplemental oxygen.
📍
High V/Q units (ventilation > perfusion) represent dead space, increasing ventilatory demand.
📍
Shunt represents V/Q = 0 (perfusion without ventilation); dead space represents V/Q = ∞.
📍
Board concept: Most lung diseases create both low and high V/Q units, but hypoxemia dominates.
Three-Compartment Model of Gas Exchange
🔹
Compartment 1: Normal V/Q units with matched ventilation and perfusion
🔹
Compartment 2: Shunt units (V/Q = 0) where blood bypasses gas exchange entirely
🔹
Compartment 3: Dead space units (V/Q = ∞) where ventilation is wasted
🔹
Total PaO₂ = weighted average of all compartments based on their blood flow contribution.
🔹
Shunt has disproportionate effect because deoxygenated blood dramatically lowers the average.
🔹
Board principle: Small shunts cause large drops in PaO₂; large dead space causes minimal hypoxemia.

Hypercapnia and the Alveolar Gas Equation
⭐
Hypercapnia always decreases PAO₂ through direct displacement in the equation.
⭐
Acute hypercapnia: PaCO₂ 40→60 mmHg reduces PAO₂ by 25 mmHg.
⭐
Chronic hypercapnia with metabolic compensation maintains near-normal pH but persistently low PAO₂.
⭐
Permissive hypercapnia in ARDS accepts higher PaCO₂ to avoid ventilator-induced lung injury.
⭐
Board distinction: Acute vs chronic hypercapnia distinguished by pH and bicarbonate compensation.

Mixed Venous Oxygen and Shunt Physiology
✅
Mixed venous PO₂ (PvO₂) normally ≈40 mmHg, reflecting tissue extraction.
✅
In pure shunt, arterial PO₂ approaches mixed venous PO₂ as shunt fraction increases.
✅
Decreased cardiac output → lower PvO₂ → worsened hypoxemia through shunted blood.
✅
Increased oxygen consumption (fever, seizures) → lower PvO₂ → magnified shunt effect.
✅
Board concept: Shunt-related hypoxemia worsens with decreased cardiac output or increased metabolism.

Oxygen Content vs Partial Pressure
🧠
Oxygen content = (1.34 × Hgb × SaO₂) + (0.003 × PaO₂)
🧠
>98% of oxygen is bound to hemoglobin; dissolved oxygen contributes minimally.
🧠
Anemia decreases oxygen content despite normal PaO₂ and saturation.
🧠
Carbon monoxide shifts the oxyhemoglobin curve leftward and decreases oxygen-carrying capacity.
🧠
Board distinction: Hypoxemia (low PaO₂) vs hypoxia (inadequate tissue oxygen delivery).

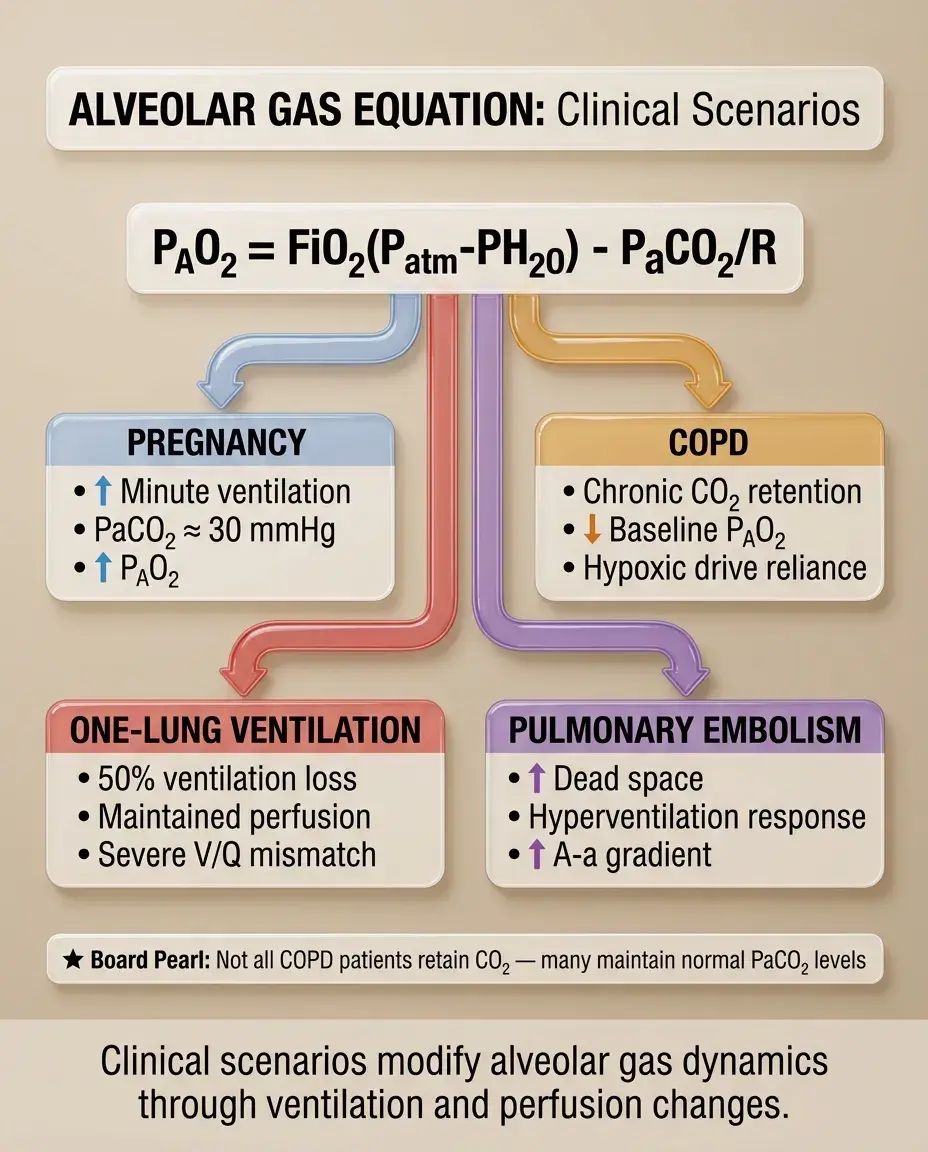
Special Scenarios Affecting the Alveolar Gas Equation
⚡
Pregnancy: increased minute ventilation → lower PaCO₂ (≈30) → higher PAO₂
⚡
COPD: chronic CO₂ retention → lower baseline PAO₂ → rely on hypoxic drive
⚡
One-lung ventilation: halved ventilation with maintained perfusion → significant V/Q mismatch
⚡
Pulmonary embolism: increased dead space → hyperventilation → low PaCO₂ but elevated A-a gradient
⚡
Board warning: Don't assume all COPD patients are CO₂ retainers; many maintain normal PaCO₂.
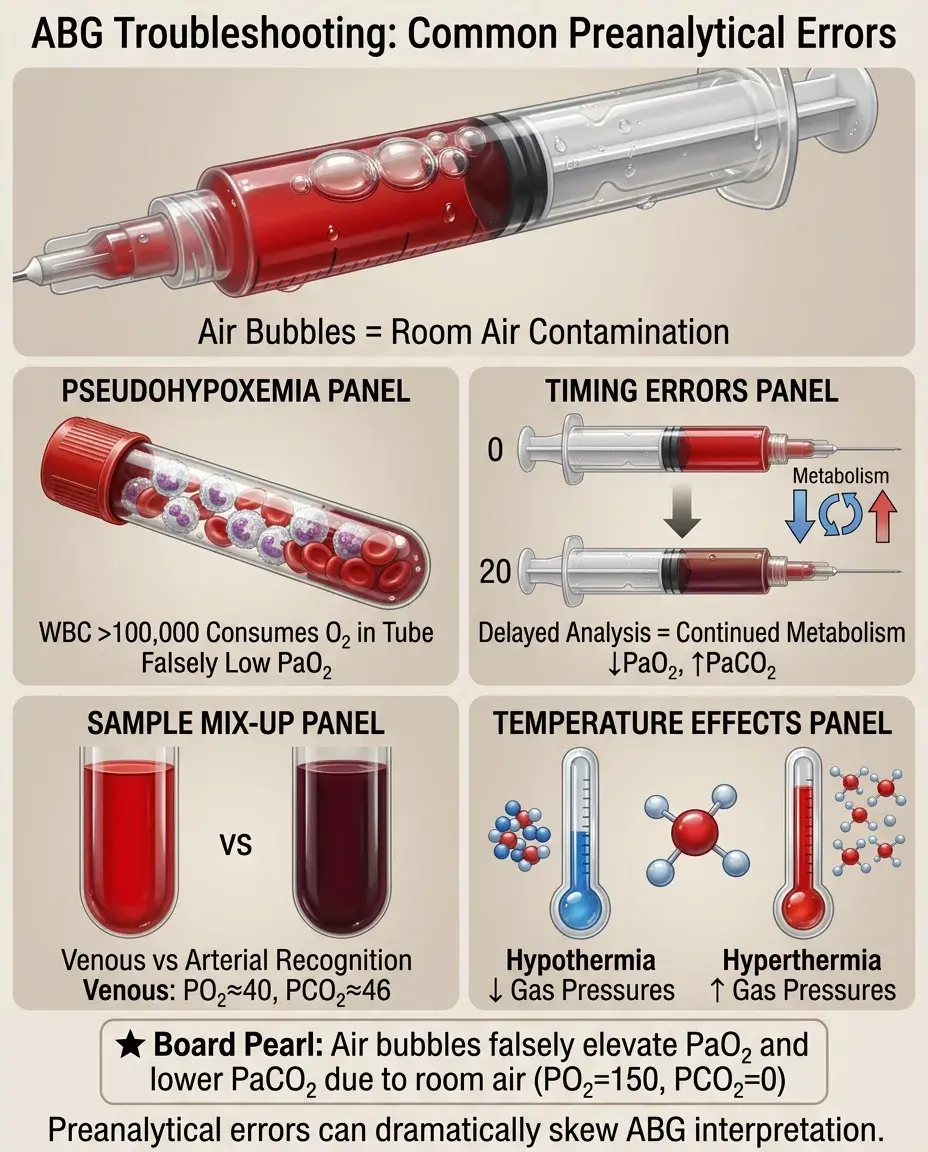
Troubleshooting Discrepancies
📌
Pseudohypoxemia: leukocytosis (>100,000) consumes oxygen in the sample → falsely low PaO₂
📌
Air bubbles in ABG: room air contamination → falsely elevated PaO₂, falsely low PaCO₂
📌
Delayed analysis: cellular metabolism continues → falsely low PaO₂, falsely high PaCO₂
📌
Venous sample mistaken for arterial: very low PO₂ (≈40), high PCO₂ (≈46)
📌
Temperature correction: hypothermia decreases gas partial pressures; hyperthermia increases them.
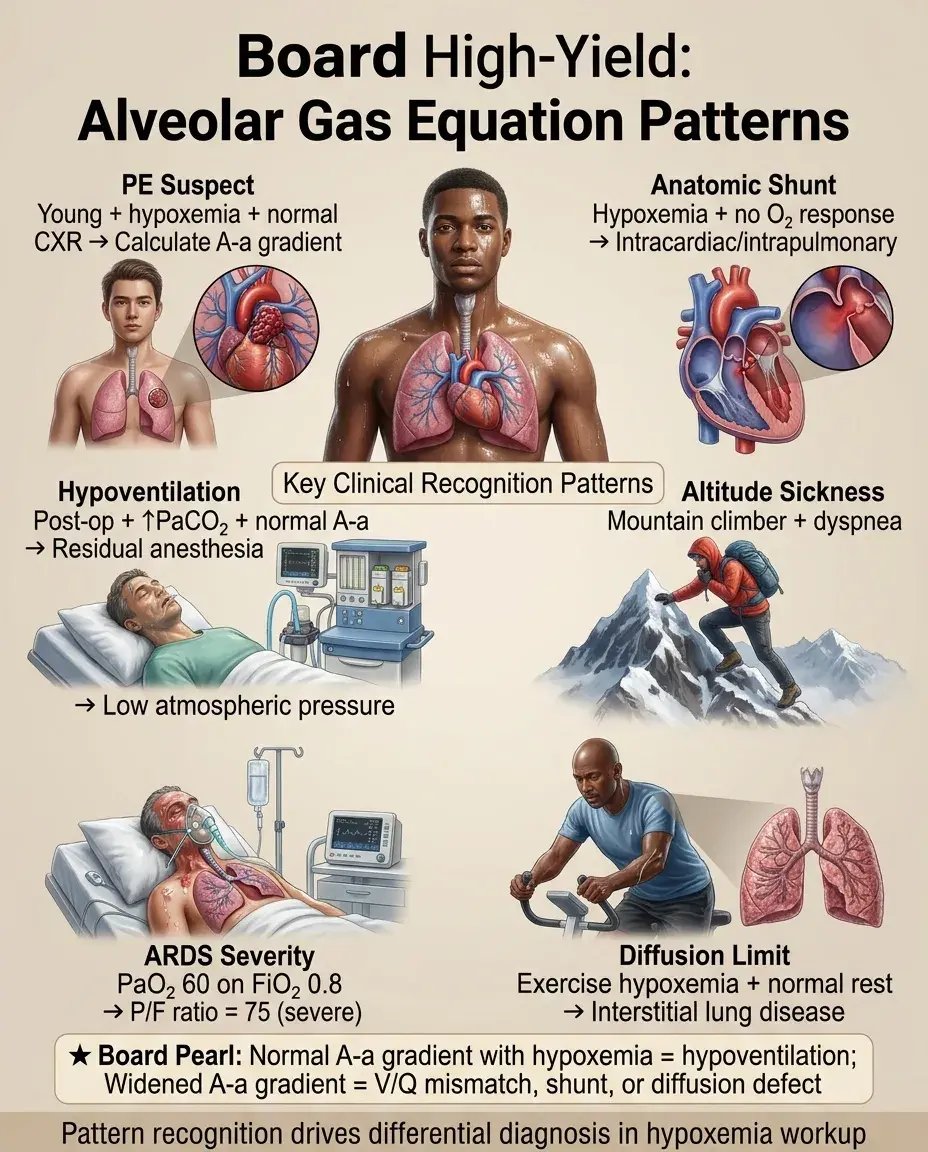
Board Question Stem Patterns
📣
Young patient with hypoxemia and normal chest X-ray → calculate A-a gradient to evaluate for PE.
📣
Hypoxemia that doesn't improve with 100% oxygen → anatomic shunt (intracardiac or intrapulmonary).
📣
Post-operative hypoxemia with elevated PaCO₂ and normal A-a gradient → hypoventilation from residual anesthesia.
📣
Mountain climber with dyspnea → low atmospheric pressure causing hypoxemia despite hyperventilation.
📣
ARDS patient with PaO₂ 60 on FiO₂ 0.8 → P/F ratio 75 indicates severe ARDS.
📣
Exercise-induced hypoxemia with normal resting saturation → diffusion limitation from ILD.
One-Line Recap
🔸
The alveolar gas equation (PAO₂ = FiO₂[Patm − PH₂O] − PaCO₂/RQ) quantifies available alveolar oxygen, enabling calculation of the A-a gradient to distinguish gas exchange abnormalities (elevated gradient) from hypoventilation or low inspired oxygen (normal gradient), thereby systematically approaching hypoxemia on board examinations.

bottom of page