top of page

eduo
visual

Human Development & Aging
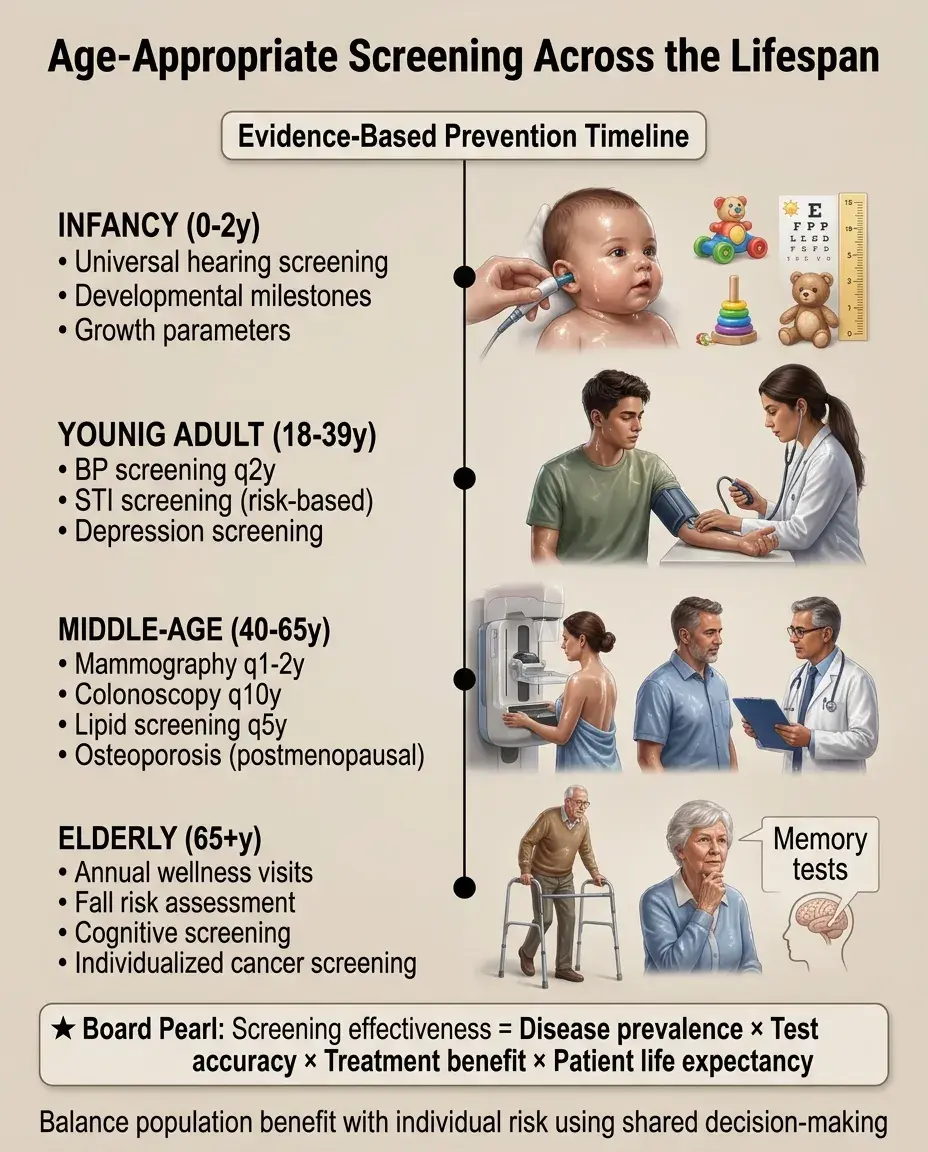
Age-appropriate screening (BP, lipid, cancer, osteoporosis)
Core Principle of Age-Appropriate Screening
🧷
Screening aims to detect disease in asymptomatic individuals when early intervention improves outcomes — the foundation is that earlier detection leads to better prognosis.
🧷
Effective screening requires: high disease prevalence in target population, available effective treatment, acceptable test characteristics (sensitivity/specificity), and favorable benefit-to-harm ratio.
🧷
Age-based recommendations balance disease incidence curves with life expectancy and competing mortality risks.
🧷
Board pearl: Screening guidelines change based on risk factors — family history, ethnicity, and comorbidities modify standard age cutoffs.

Blood Pressure Screening Guidelines
📍
Adults ≥18 years: BP screening at every healthcare encounter or at least annually if normal (<120/80).
📍
Children ≥3 years: annual BP screening at well-child visits.
📍
Diagnosis requires elevated readings on ≥2 separate occasions using proper technique (correct cuff size, seated 5 minutes, arm at heart level).
📍
Stage 1 HTN: 130-139/80-89; Stage 2 HTN: ≥140/90.
📍
Board distinction: Screening detects HTN, but diagnosis requires confirmation — a single elevated reading is insufficient for diagnosis or treatment initiation.

Lipid Screening Across the Lifespan
🔹
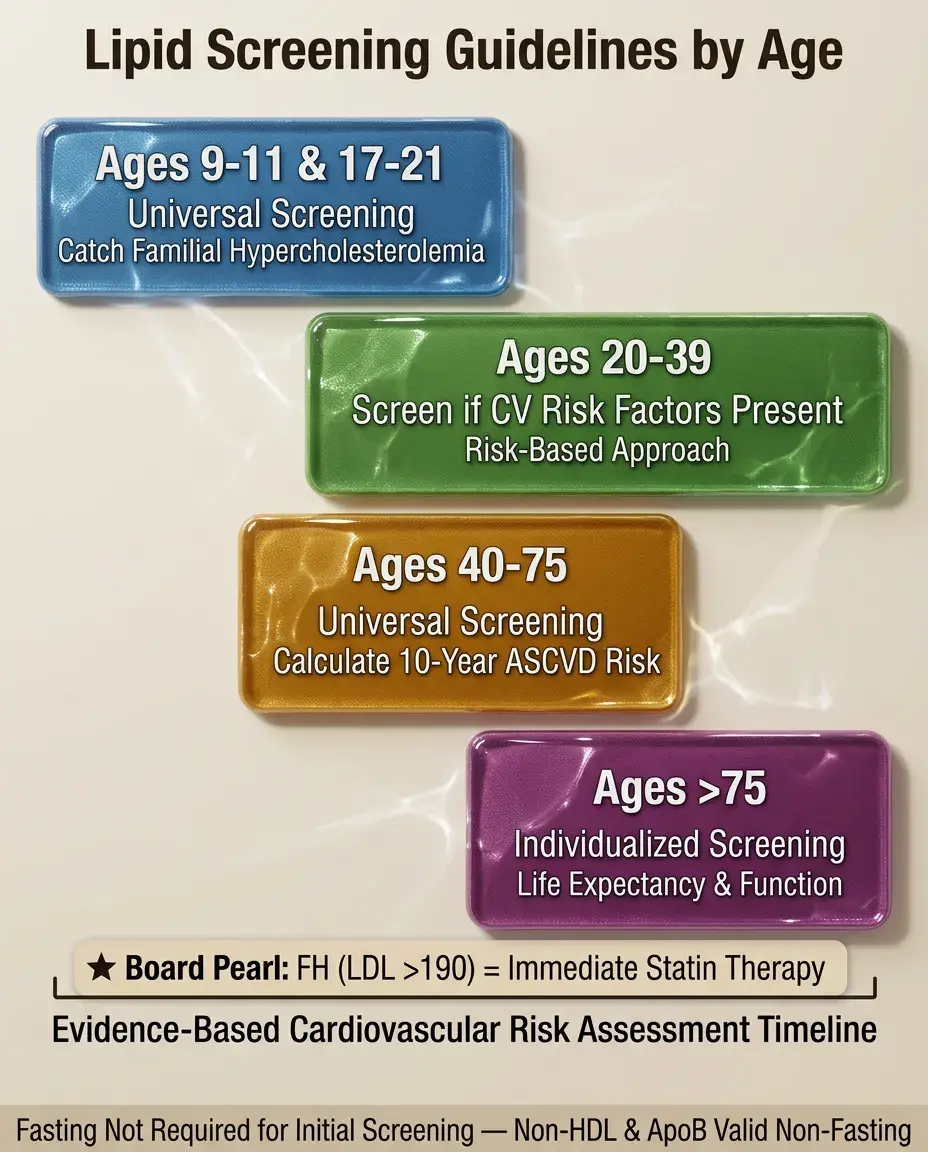
Universal pediatric screening: ages 9-11 and 17-21 (catch familial hypercholesterolemia).
🔹
Adults 20-39: screen if cardiovascular risk factors present.
🔹
Adults 40-75: universal screening to calculate 10-year ASCVD risk.
🔹
Adults >75: individualized based on life expectancy and functional status.
🔹
Fasting not required for initial screening — non-HDL cholesterol and apoB are valid non-fasting.
🔹
Board pearl: Familial hypercholesterolemia (LDL >190) warrants immediate statin therapy regardless of calculated risk.
Breast Cancer Screening Controversies
⭐
Mammography starting age varies by organization: USPSTF says 50, ACS says 45, ACOG says offer at 40.
⭐
Ages 50-74: biennial mammography has strongest evidence (USPSTF Grade B).
⭐
Ages 40-49: shared decision-making based on individual risk/benefit (USPSTF Grade C).
⭐
Clinical breast exam: no proven mortality benefit when added to mammography.
⭐
Board clue: Dense breast tissue reduces mammography sensitivity — supplemental ultrasound or MRI may be indicated.
⭐
BRCA carriers: annual MRI starting age 25-30 plus mammography starting age 30.

Cervical Cancer Screening Evolution
✅
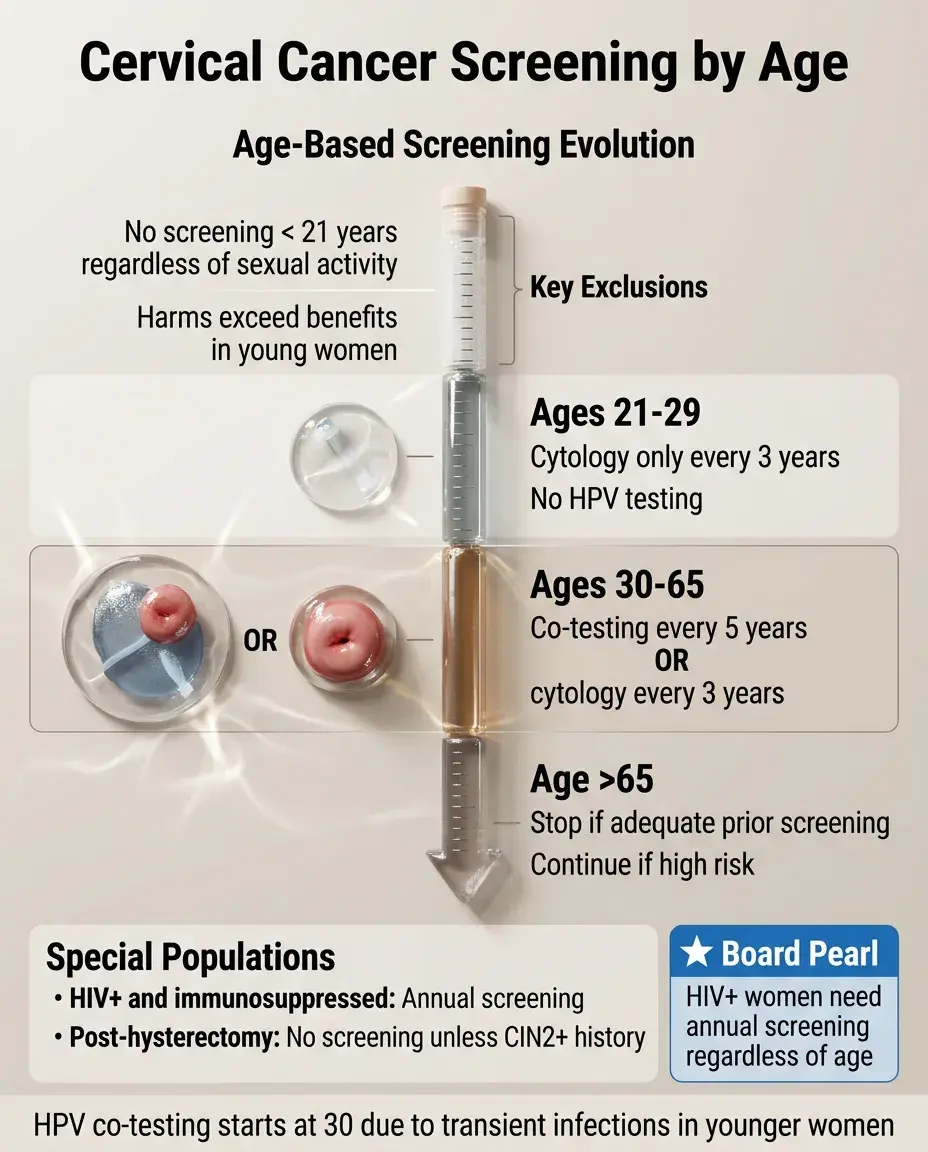
Age 21-29: cytology alone every 3 years (HPV testing not recommended due to high transient infection rate).
✅
Age 30-65: co-testing (cytology + HPV) every 5 years OR cytology alone every 3 years.
✅
No screening <21 years regardless of sexual activity — harms exceed benefits.
✅
No screening >65 if adequate prior screening and not high risk.
✅
Board pearl: HIV+ and immunosuppressed women need annual screening.
✅
Post-hysterectomy with cervix removal: no screening unless history of CIN2+ or cervical cancer.
Colorectal Cancer Screening Options
🧠
Average risk screening starts age 45 (lowered from 50 due to rising young-onset CRC).
🧠
Options: colonoscopy q10 years, annual FIT, FIT-DNA q3 years, flexible sigmoidoscopy q5 years, CT colonography q5 years.
🧠
High-risk groups start earlier: family history of CRC <60 or advanced adenoma → start at 40 or 10 years before youngest affected relative.
🧠
Board distinction: Positive non-colonoscopy test → diagnostic colonoscopy required (not screening).
🧠
IBD patients: colonoscopy beginning 8 years after diagnosis with surveillance based on findings.

Lung Cancer Screening Criteria
⚡
Annual low-dose CT for ages 50-80 with 20 pack-year history AND current smoker or quit within 15 years.
⚡
Discontinue when >15 years quit, life expectancy <10 years, or inability to undergo curative surgery.
⚡
Number needed to screen to prevent one death: ~320 (comparable to mammography).
⚡
Board pearl: Incidental nodules are common (~25%) — Lung-RADS classification guides follow-up.
⚡
Shared decision-making required due to false positive rate, radiation exposure, and overdiagnosis risk.

Prostate Cancer Screening Debate
📌
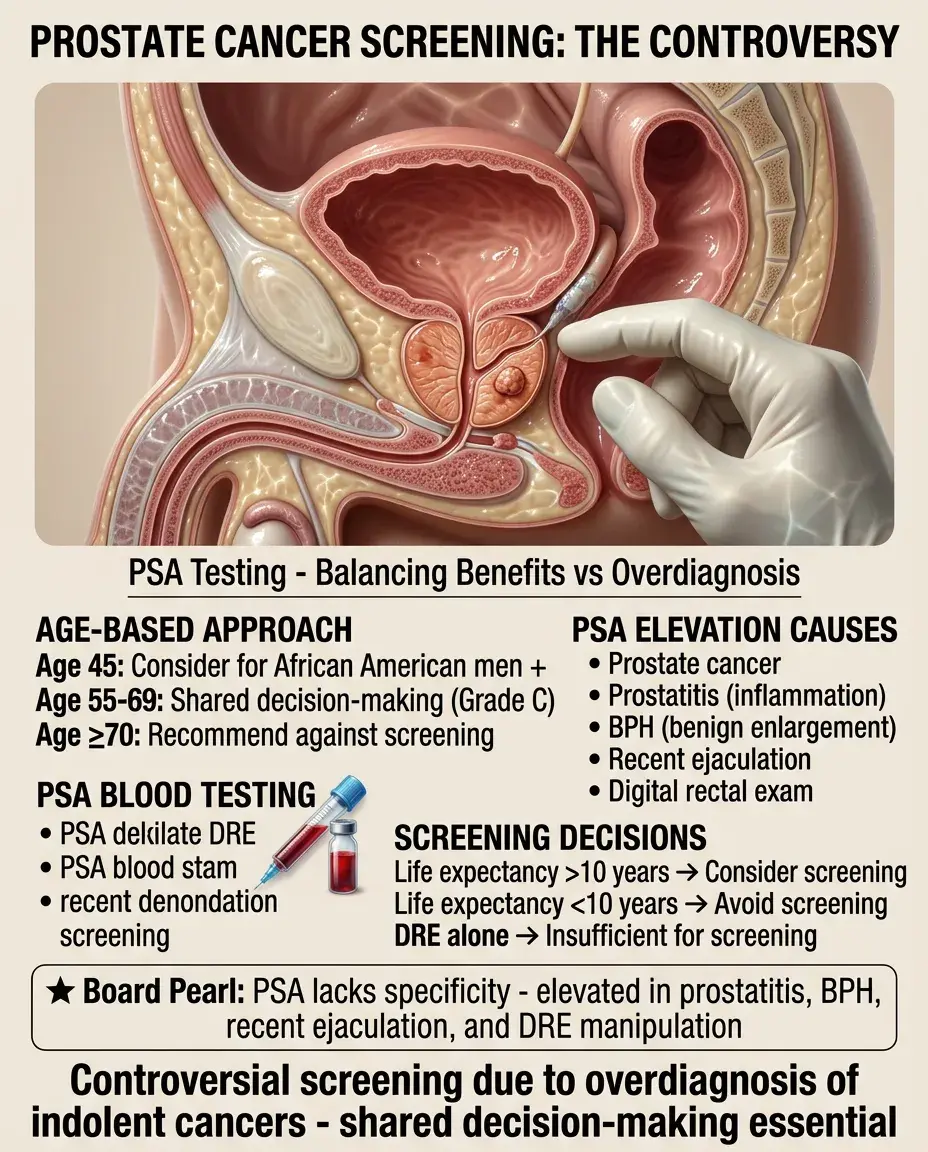
PSA screening remains controversial due to overdiagnosis and overtreatment of indolent cancers.
📌
Age 55-69: shared decision-making about PSA screening (USPSTF Grade C).
📌
Age ≥70 or life expectancy <10 years: recommend against screening.
📌
African American men and those with family history: consider starting at age 45.
📌
Board clue: PSA can be elevated by prostatitis, BPH, recent ejaculation, or prostate manipulation — not specific for cancer.
📌
Digital rectal exam alone is insufficient for screening.
Osteoporosis Screening and FRAX
📣
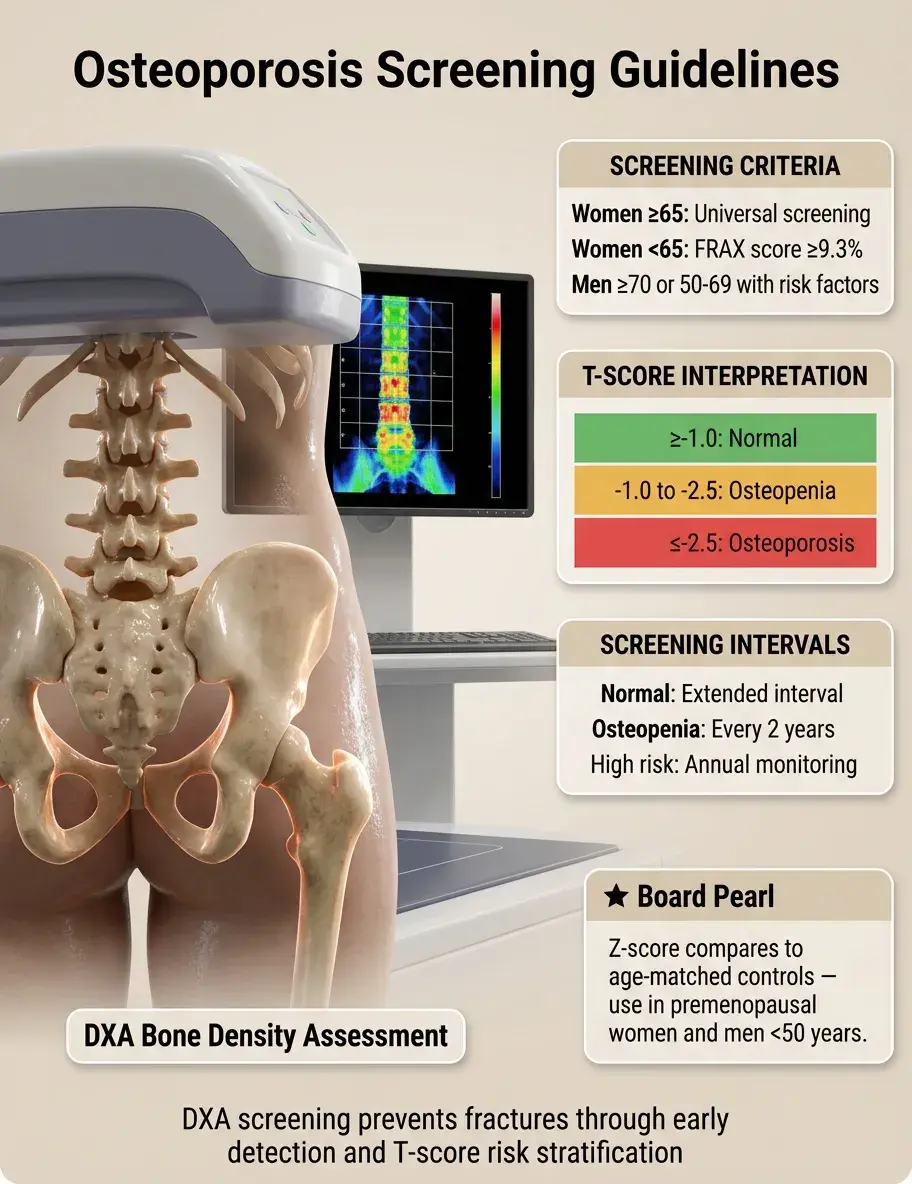
Women ≥65 years: universal bone density screening (DXA scan).
📣
Women <65: screen if 10-year fracture risk equals that of 65-year-old (FRAX score ≥9.3%).
📣
Men ≥70 or men 50-69 with risk factors (prior fracture, glucocorticoid use, hypogonadism).
📣
T-score interpretation: ≥-1.0 normal, -1.0 to -2.5 osteopenia, ≤-2.5 osteoporosis.
📣
Board pearl: Z-score compares to age-matched controls — used in premenopausal women and men <50.
📣
Screening interval: 2 years for osteopenia, longer if normal initial scan.
Diabetes Screening Thresholds
🔸
Adults ≥35 years: universal screening regardless of risk factors (ADA 2022 update).
🔸
Any age with BMI ≥25 (≥23 in Asians) plus one risk factor: family history, high-risk ethnicity, PCOS, physical inactivity.
🔸
Women with gestational diabetes: lifelong screening every 3 years.
🔸
Prediabetes (A1c 5.7-6.4%, FPG 100-125, OGTT 140-199): annual screening.
🔸
Board distinction: Screening tests are fasting glucose, A1c, or OGTT — all are acceptable.
🔸
Children: screen if BMI ≥85th percentile plus two risk factors starting at age 10 or puberty.

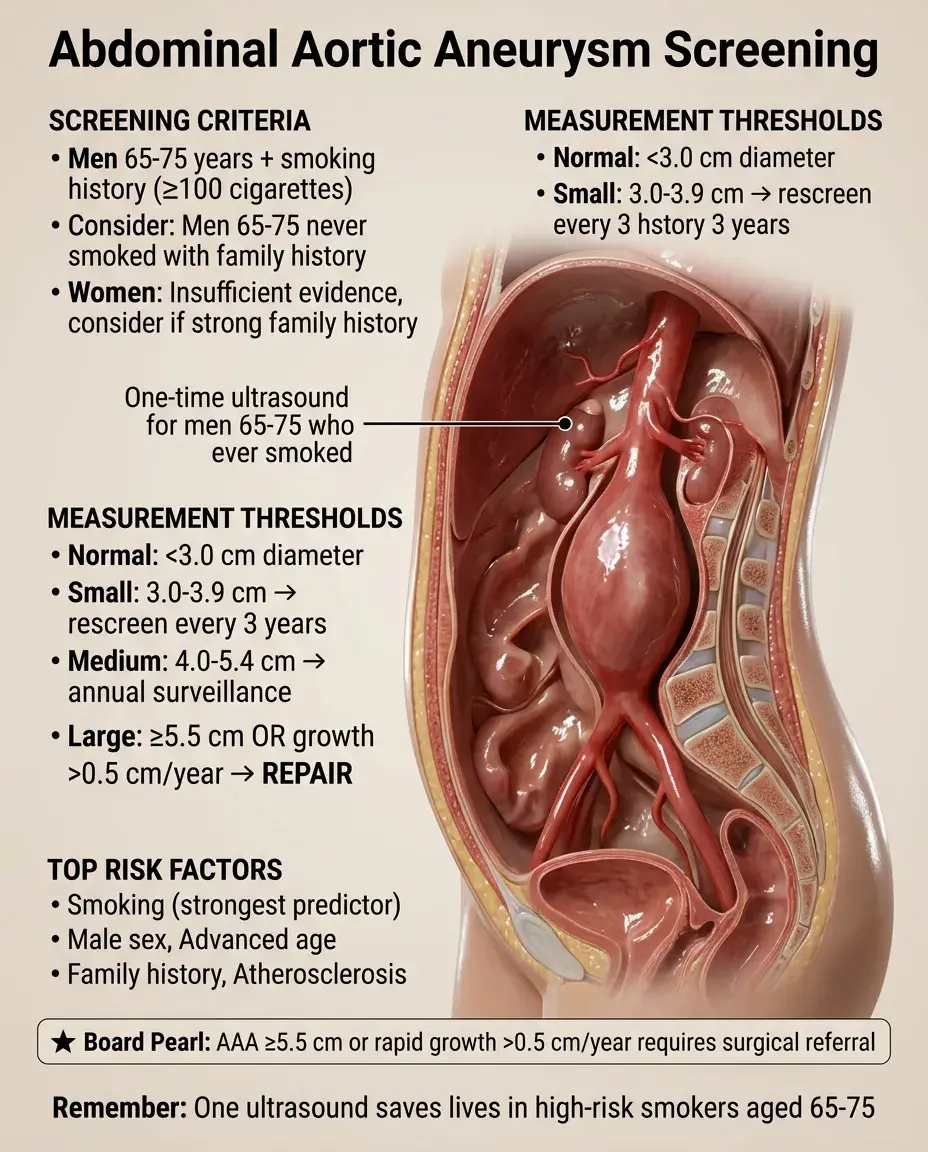
Abdominal Aortic Aneurysm Screening
🧷
One-time ultrasound screening for men aged 65-75 who have ever smoked (≥100 lifetime cigarettes).
🧷
Consider screening men 65-75 who never smoked based on family history and individual risk.
🧷
Women who have smoked: insufficient evidence, but consider if strong family history.
🧷
Board pearl: Aneurysm ≥5.5 cm or growing >0.5 cm/year → refer for repair.
🧷
Follow-up surveillance: 3.0-3.9 cm every 3 years, 4.0-5.4 cm annually.
🧷
Risk factors: smoking (strongest), male sex, age, family history, atherosclerosis.
Hepatitis Screening Populations
📍
HCV: one-time screening for all adults 18-79 regardless of risk (major guideline change).
📍
HBV: screen high-risk groups — IV drug users, MSM, HIV+, household contacts of HBV+, hemodialysis, elevated ALT, pregnant women.
📍
Born in HBV-endemic areas (Asia, Africa, Pacific Islands): screen regardless of vaccination status.
📍
Board clue: HCV screening uses antibody test → if positive, confirm with HCV RNA.
📍
HBV screening includes HBsAg and anti-HBs (anti-HBc if from endemic area).
📍
Pregnant women: universal HBV screening, HCV if risk factors.

HIV Screening Recommendations
🔹
Universal opt-out screening for all patients aged 13-64 at least once.
🔹
Annual screening for high-risk groups: MSM, IV drug users, sexually active with HIV+ partner.
🔹
Pregnant women: screen at first prenatal visit, retest in third trimester if high risk.
🔹
Fourth-generation combination antigen/antibody test detects infection earlier than antibody alone.
🔹
Board pearl: Acute HIV may present with negative antibody but positive viral load — consider in mononucleosis-like illness with risk factors.
🔹
PrEP candidates need baseline HIV testing plus regular monitoring.

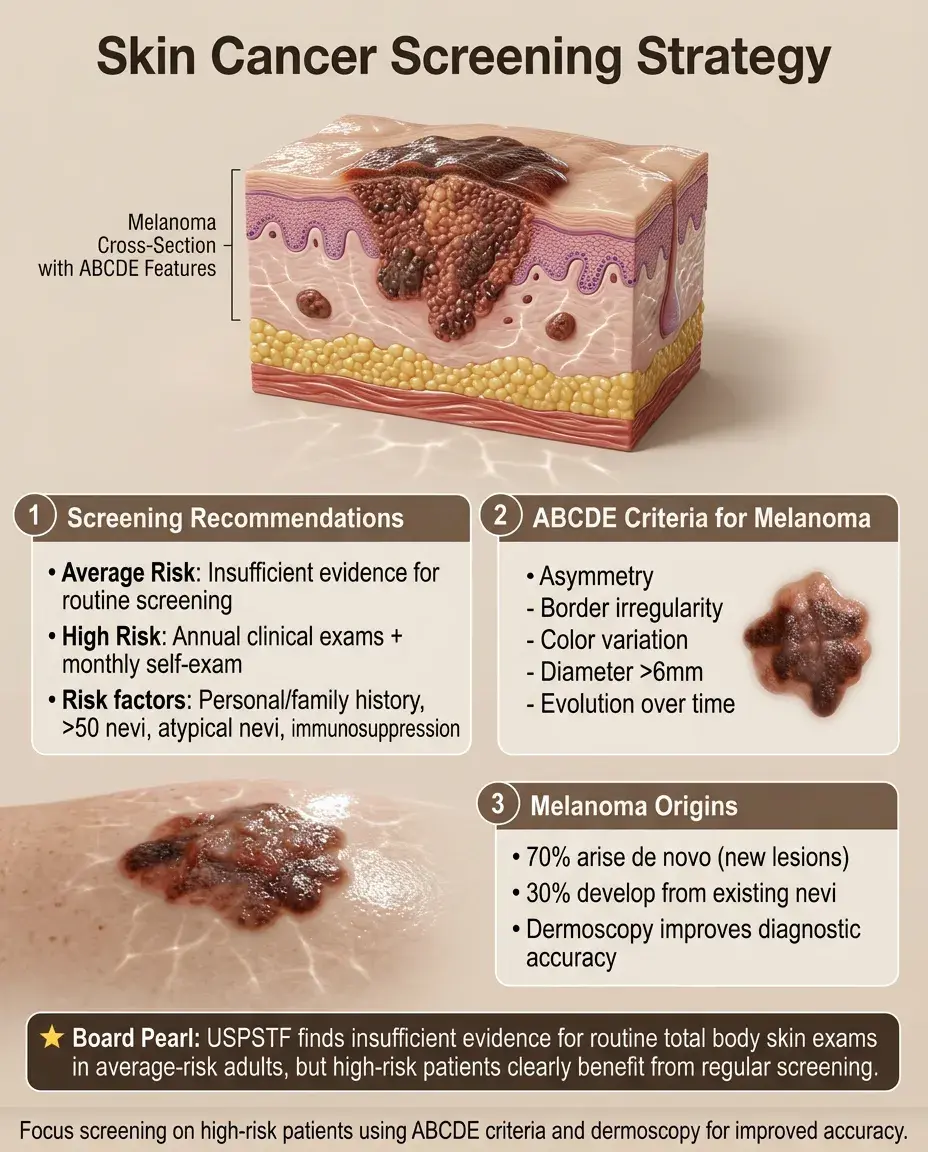
Skin Cancer Screening Approach
⭐
USPSTF: insufficient evidence for routine total body skin exams in average-risk adults.
⭐
High-risk patients benefit from screening: personal history of skin cancer, family history of melanoma, >50 nevi, atypical nevi, immunosuppression.
⭐
ABCDE criteria: Asymmetry, Border irregularity, Color variation, Diameter >6mm, Evolution.
⭐
Board distinction: Melanoma can arise de novo (70%) or from existing nevi (30%).
⭐
Dermoscopy by trained providers increases diagnostic accuracy.
⭐
Patient self-examination monthly with annual clinical exams for high-risk individuals.
Thyroid Disease Screening
✅
No routine TSH screening in asymptomatic adults (USPSTF recommendation).
✅
Consider screening in high-risk groups: women >60, family history, autoimmune disease, Down syndrome, Turner syndrome.
✅
Pregnancy: universal TSH screening at first prenatal visit if symptomatic or risk factors.
✅
Subclinical hypothyroidism (elevated TSH, normal T4): found in 4-8% of adults, treatment controversial.
✅
Board pearl: Lithium, amiodarone, and radiation exposure warrant periodic thyroid monitoring.
✅
Neck radiation in childhood: annual thyroid palpation starting 5 years post-exposure.

Depression and Anxiety Screening
🧠
Adults: screen for depression in settings with adequate support systems for diagnosis and treatment.
🧠
Adolescents 12-18: screen for major depressive disorder annually.
🧠
Pregnant and postpartum women: screen during pregnancy and postpartum period.
🧠
Common tools: PHQ-2 (initial), PHQ-9 (follow-up), Edinburgh Postnatal Depression Scale.
🧠
Board distinction: Positive screen requires clinical interview for diagnosis — screening tools alone don't diagnose.
🧠
Elderly: use Geriatric Depression Scale (yes/no format easier for cognitive impairment).
🧠
Anxiety screening gaining support but not yet universally recommended.

Sexually Transmitted Infection Screening
⚡
Chlamydia/gonorrhea: annual screening for sexually active women ≤24, older women with risk factors, MSM.
⚡
Syphilis: screen pregnant women, MSM, HIV+, commercial sex workers.
⚡
Pregnancy STI panel: HIV, HBV, syphilis, chlamydia/gonorrhea if <25 or risk factors.
⚡
Board pearl: Nucleic acid amplification tests (NAAT) preferred for chlamydia/gonorrhea — can use urine, cervical, vaginal, pharyngeal, rectal specimens.
⚡
Expedited partner therapy: prescribe treatment for partners without examination (legal in most states).
⚡
Three-site testing (pharynx, rectum, urine/genital) for MSM given varied sexual practices.

Vision and Hearing Screening
📌
Newborns: red reflex exam to detect cataracts, universal hearing screening before discharge.
📌
Children: vision screening at 3, 4, 5 years then annually; formal audiometry if failed screening.
📌
Adults 18-39: comprehensive eye exam based on risk factors.
📌
Adults ≥65: annual eye exams for glaucoma, macular degeneration, cataracts.
📌
Board clue: Amblyopia screening critical before age 5 — after this, vision loss may be permanent.
📌
Diabetics: dilated eye exam within 5 years of type 1 diagnosis, at type 2 diagnosis, then annually.
📌
Hearing loss in elderly associated with cognitive decline, depression, falls.

Board Question Stem Patterns
📣
52-year-old woman asks about mammography → discuss shared decision-making for ages 40-49.
📣
28-year-old woman with ASCUS Pap → HPV testing determines colposcopy need.
📣
45-year-old man with 25 pack-year smoking history → too young for lung cancer screening (start at 50).
📣
68-year-old woman never screened for osteoporosis → order DXA scan.
📣
22-year-old sexually active woman → annual chlamydia screening indicated.
📣
40-year-old with BMI 28 and family history of diabetes → screen now, don't wait until 45.
📣
One-time positive BP reading of 142/88 → recheck before diagnosing hypertension.

One-Line Recap
🔸
Age-appropriate screening balances disease prevalence, test characteristics, and life expectancy across the lifespan — from universal newborn hearing screening through risk-stratified cancer screening in adults — with guidelines evolving based on epidemiologic trends, requiring clinicians to individualize recommendations using shared decision-making for controversial screens while maintaining population health through evidence-based protocols.
bottom of page